The task force chairmen, steering committee members, and participants remind readers of this report that the affiliations of the contributors are listed only for identification and that they do not imply institutional endorsement. Contributors to this report do not necessarily represent their institutions, and every member of the task force does not necessarily endorse every recommendation made in this report
Executive Summary
This report presents the observations, findings, and recommendations of a task force formed to examine the global response and the response of the U.S. government (USG) to the 2013–2014 Ebola outbreak and global transmission. Specifically, the task force sought to derive lessons learned and insights from the USG response to the Ebola outbreak both internationally and domestically with the goal of crafting recommendations to improve the government’s ability to respond to natural disasters, acts of bioterrorism, and various public health crises related to significant outbreaks, epidemics, and pandemics.
The task force included homeland security experts and representatives from academia, research institutions, and the private sector. The task force evaluated the USG response—particularly by the Department of Health and Human Services (HHS) and the Department of Homeland Security (DHS)—to the outbreak and global transmission of the Ebola virus disease (EVD). It drew findings from in-depth observations and developed a series of recommendations for improving the U.S. response to disasters.
These observations, findings, and recommendations make the case for reorganizing existing relief systems and improving emergency preparedness across the spectrum. Additionally, the task force concluded that a government response that focused on enabling and empowering professionals by providing the required knowledge and the statutory mandate for leadership to manage the crisis effectively, coupled with a uniform response structure regardless of the nature of the emergency, would allow for improved, coordinated responses with focused messaging. Focused messaging was generally lacking in the USG response during the outbreak.
Each section of this report includes a series of observations, findings, and recommendations formulated by members of the task force. The report’s major recommendations include:
- Prioritize emergency preparedness and planning. Speedy, comprehensive, preplanned responses coordinated among various levels of government, international organizations, domestic and international nongovernmental aid organizations, and the private sector can quickly mitigate and contain the spread of EVD and other highly contagious pathogens. The planning should identify medical facilities, personnel with the necessary expertise, and the appropriate medical supplies well in advance and predesignate specific agencies to coordinate and lead the national response.
- Empower officials to coordinate domestic response efforts and communicate with the American public. The officials responsible for coordinating the federal response on behalf of the President must be actively engaged with federal, state, and local officials and the private sector, providing leadership during the crisis. The officials must also effectively communicate with the American public by employing carefully crafted risk messaging that contains rational, evidence-based information and guidance, and instructions on steps the public should take to prepare for and to prevent epidemic spread.
- Improve medical training and increase access to effective and sustainable health care for West African countries. Globalization has lifted countries out of poverty and has improved the quality of life for hundreds of millions of people, but it has also enabled greater spread of diseases that were previously contained to remote parts of the world. It is therefore in the American interest to support improved medical care, especially in vulnerable countries. This can be accomplished by installing free trade and free-market institutions, which can enable enhanced access to Western medical supplies. Building an indigenous capacity to import and distribute desperately needed medical supplies will not only greatly enhance quality of life in West Africa, but also create a new market for vaccine and medicine manufacturers. In this endeavor, every element—the private sector, nongovernmental organizations (NGOs), international organizations, and governments—will have a role to play.
- Strengthen lines of authority and narrow the priorities of the World Health Organization (WHO) to focus on a limited number of core responsibilities. Politicization within the organization and inefficient lines of authority severely limited WHO’s ability to respond swiftly and effectively to the EVD outbreak in West Africa. Serious reforms must be implemented to ensure the agency does not continue to fumble in potentially catastrophic public health emergencies. WHO must remain focused on its core competencies: building the capacity of national health systems in developing countries and monitoring and coordinating the international response to epidemic disease.
Congress and the Administration should develop a comprehensive plan to implement these recommendations to ensure that the USG—specifically HHS and DHS—are better prepared to respond to future crises and to protect the American public.
Introduction
In September 1976, scientists in Antwerp’s Institute of Tropical Medicine received a package from a Belgian doctor working in Yambuka, Zaire (now the Democratic Republic of the Congo or DRC). It contained blood samples from a Belgian nun who had contracted and died from a mysterious disease that had devastated the community.[1] They first thought that the nun died from yellow fever, but testing of the samples revealed an unknown disease that was eventually named after Ebola, a local river near Yambuka.[2] The Dutch researchers who travelled to the site concluded that the disease was spreading due to the reuse of syringes and washing of dead bodies—meaning that it was being passed via bodily fluids, not through the air.[3]
Since 1976, three strains of Ebola virus (Zaire, Sudan, and Bundibugyo) have caused 24 separate outbreaks of varying severity, predominantly in small central African towns and villages. All of the Ebola outbreaks remained localized, resulting in 2,387 confirmed cases and 1,590 confirmed deaths as of September 2014. These outbreaks occurred in the Congo, the DRC, Gabon, Sudan, and Uganda.[4] In 1989, a new strain of Ebola virus disease (EVD) was detected in Reston, Virginia. This strain materialized in association with an outbreak in monkeys that had been imported to the United States from the Philippines without evidence of human illness.[5] Other isolated cases have occurred elsewhere, related to laboratory accidents, travel, or health care–acquired infection. In 1994, the Tai Forest strain of the virus caused an isolated case of infection in a scientist studying an outbreak among chimpanzees.
The most recent outbreak due to the Zaire strain began in Guinea in December 2013, spreading to the adjacent countries of Sierra Leone and Liberia. The current outbreak is the first Ebola outbreak in West Africa and the worst since the disease was discovered in 1976, causing more cases and deaths than all other outbreaks of the disease combined.[6]
The current West Africa EVD epidemic has been traced back to Emile Ouamouno, a two-year-old boy in the village of Meliandou in southeastern Guinea.[7] The child (the “index patient” or “patient zero”) died on December 6, 2013, just four days after showing symptoms and seems to have passed the disease to his mother, three-year-old sister, and grandmother—all of whom later died of the disease. The village midwife was also hospitalized and later died. In each case the victims suffered from fever, vomiting, and diarrhea, but the presence of Ebola was still unknown. Two people who attended the grandmother’s funeral are believed to have contracted the disease and taken it with them when they returned home to their village.[8]
The disease continued to spread, but not until late March 2014, some 15 weeks after the first death, did hospital staff in Guinea—which had never seen EVD before—report suspected cases to Guinea’s Ministry of Health and Médecins Sans Frontières (Doctors Without Borders or MSF). By then the epidemic was out of control. New cases were soon reported in several different parts of Guinea and in neighboring Sierra Leone. By March 2014, MSF declared that the current outbreak was “unprecedented” and warned of the difficulties in combatting the disease in multiple locations.[9] Prior to the deaths in a rural prefecture of Guinea, EVD was primarily found in Central Africa. The misdiagnosis was the spark that ignited an international epidemic that has ravaged the nations of Guinea, Sierra Leone, and Liberia and has ignited a firestorm of press, protest, and policy conundrums for countries around the world.
One likely reason for this outbreak’s extensive and rapid spread and the high body count is that the virus spread to major cities. Overcrowding and poor sanitation in the cities allowed EVD to spread more extensively than in earlier cases, where the virus burned itself out in small, isolated villages. By early April, Guinea had confirmed EVD cases in Conakry, its capital.[10] By June, EVD had reached Monrovia, Liberia’s capital.[11] Although medical facilities may be better in cities, contact tracing and containment are more difficult. The costs for failing to contain the disease became evident in the summer of 2014, when health workers struggled to wear adequate personal protective equipment (PPE) in the searing summer heat. On July 29, 2014, Dr. Sheik Umar Khan, the health official leading Sierra Leone’s fight against the epidemic, became the most prominent of the hundreds of health workers who died fighting the virus.
The governments of Guinea, Liberia, and Sierra Leone strove to prevent the spread of the disease by issuing public health warnings about how the virus spreads, urging people to remain at home, closing schools, imposing military-enforced quarantines and curfews, and partially closing their international borders. Nonetheless, in July 2014, the virus spread further when Patrick Sawyer, an infected Liberian diplomat, arrived in Nigeria by plane and died. Several other cases were soon reported in Nigeria. EVD later appeared in Senegal. Compared with its quick spread in several other countries, Nigeria’s experience with Ebola was quite mild with only seven Nigerians dying from the disease. The last confirmed case of EVD in Nigeria occurred on September 5, 2014. As per the World Health Organization (WHO) policies, which define an outbreak as “over” if a country has not reported a new case after two successive incubation periods of 21 days, Nigeria was declared Ebola-free in late October, as was Senegal.[12] Shortly thereafter, the Mali Health Minister announced that a two-year-old foreign girl had brought the virus to Mali.[13]
Globalization brought Ebola to the United States via Thomas Eric Duncan, a Liberian national who traveled to Dallas to visit his family. He left Liberia on September 19 after passing a fever check at the airport and arrived in Dallas the next day. He developed symptoms days later and went to Texas Health Presbyterian Hospital on September 25, only to be sent home despite doctors knowing that he had recently arrived from West Africa. He was brought back to the hospital on September 28 and put into isolation. He died on October 8.[14]
In the United States, 48 people are believed to have been exposed to Duncan when he might have been contagious. Of those, 43 were cleared.[15] However, Texas Health Presbyterian Hospital now appears to have been unprepared to deal with EVD because two nurses were later diagnosed with the disease. One nurse, Amber Joy Vinson, had traveled out of state. At the time of her flight, she reported to the Centers for Disease Control and Prevention (CDC) that she had a fever, but because it was only 99.5, not above the established alert threshold of 100.4, the CDC cleared her to take a commercial flight.[16]
Duncan’s entrance into the United States and the infection of two of his nurses galvanized public fears of Ebola. Many criticized the lackluster standards and procedures that they saw as leading to both EVD’s entry into the U.S. and its spread to health care workers. The CDC issued new standards for wearing protective gear, and new screening procedures were put in place at Kennedy International, Dulles, Chicago O’Hare, Hartsfield-Jackson, and Newark Liberty airports to test the temperatures and check the travel histories of passengers who might have been in West Africa.[17] On October 22, the CDC mandated that all travelers who arrive in the United States from the West African countries with the disease be monitored by officials for a 21-day incubation period.[18] Nonetheless, at the end of October, Dr. Craig Spencer, who had returned from treating Ebola patients in West Africa with MSF, was confirmed to be infected with the virus.[19] New York and New Jersey announced more stringent regulations for doctors and nurses returning from treating EVD in West Africa. Health officials affected by the regulations have criticized them, while concerns have been raised about whether the restrictions will deter doctors and nurses from volunteering to travel to West Africa, where more health care workers are desperately needed.[20]
This report assesses the USG response to the EVD outbreak that originated in December 2013 in West Africa. Based on thorough research and in-depth analysis, the task force has developed a series of recommendations to improve the speed, efficiency, and effectiveness of the government’s response to future crises and efforts to protect the public.
Background
The Ebola Virus Disease
EVD or Ebola hemorrhagic fever causes disease in humans and nonhuman primates, such as monkeys, gorillas, and chimpanzees. Ebola belongs to the virus family Filoviridae, which has only two members: the Marburg and Ebola viruses.[21] Both attack multiple organs and can cause extreme internal and external bleeding (hemorrhaging).[22] Death can also occur as a result of severe dehydration and hypovolemic shock—a fatal drop in blood pressure due to extremely low blood volume.
Viruses do not replicate through cell division, but instead insert their own genetic sequencing into the deoxyribonucleic acid (DNA) of the host cell and subsequently hijack all cellular processes, including transcription and translation (the processes by which DNA is read and proteins are produced). In essence, the host cell becomes a factory of viral proteins. As new viral capsules are formed, they bud from the host cell, taking a part of the host cell’s outer membrane, thus cloaking themselves against detection by the host’s immune system. In some cases, the patient’s immune system can produce enough antibodies to defeat the infection. With Ebola, the virus can often reproduce so rapidly that the immune system never catches up.
The five known strains of EVD are identified by their location of origin:
- Ebola virus (Zaire ebolavirus);
- Sudan virus (Sudan ebolavirus);
- Taï Forest virus (Taï Forest ebolavirus, formerly Côte d’Ivoire ebolavirus);
- Bundibugyo virus (Bundibugyo ebolavirus); and
- Reston virus (Reston ebolavirus).[23]
The five strains do not vary greatly, except for the Reston virus, which does not cause symptoms in humans. There have been dozens of outbreaks of EVD since its identification in 1976. The Zaire and Sudan strains are especially virulent. The current outbreak in West Africa is a product of the Zaire strain.[24]
The natural host of the virus is still unknown, but researchers believe that the virus is animal-borne (zoonotic), with the virus transmitted to humans initially through the consumption of bush meat or contact with bodily fluids of infected mammals.[25] Many experts believe that the natural reservoir of the virus is the fruit bat populations of sub-Saharan Africa, and the consumption of fruit bats is considered to be a delicacy in many parts of Africa. Although cooking the bats will kill the virus, the U.N. Food and Agriculture Organization believes food preparation to be origin of contact with the virus.[26] The fruit bats travel widely, which could explain the sudden appearance of EVD in West Africa, where it has never been known before.
Once a person is infected with the disease, symptoms typically appear within eight to 10 days, although this period can range from two to 21 days.[27] Early symptoms of human infection include a high fever, severe headache, muscle aches, chills, and fatigue. Many of these early symptoms are shared with many more common illnesses—such as the flu, malaria, and typhoid fever—complicating timely, accurate diagnosis because time is wasted administering incorrect treatments, which do not help the patient.[28] Symptoms of more advanced disease include vomiting, diarrhea, rash, chest pain, cough, internal bleeding, and bleeding from the eyes and other orifices such as ears and nose.[29]
The average human fatality rate is around 50 percent, varying from 25 percent to 90 percent in past outbreaks. Unlike the common cold virus and influenza, EVD is not airborne, but spreads mostly through direct contact with the blood, body fluids, or organs of an infected person or with infected objects, such as medical supplies, clothing, and linens. Since each EVD victim can produce up to 10 liters of infectious bodily fluids (e.g., blood, sweat, semen, mother’s milk, and urine), caregivers, health workers, and family members are at high risk of infection because they are in regular contact with these infected bodily fluids.[30]
While the current incubation period for the Ebola virus averages from two to 21 days, a person does not become contagious until symptoms have become present.[31] Researchers are looking for indicators that may help them to diagnose infection before the patient starts exhibiting symptoms.[32]
The high mortality rate is one of the disease’s most alarming aspects. There is no known cure or preventative vaccine. As such, the best chance for survival once infected is early diagnosis followed by comprehensive supportive care. While diagnostic tests exist, they often result in false negatives in those who have recently begun to experience symptoms, so isolation and retesting is often the best course of action.[33] When taken early, basic steps can improve patients’ chances of survival, including oral hydration or intravenous fluid replacement, balancing electrolytes, maintaining oxygen and blood pressure levels, and treating other infections that arise.[34]
Many African countries are especially vulnerable to EVD due to their constrained ability to meet these requirements. They suffer from limited funding for public health programs, human resources challenges such as shortages of trained professionals, limited communication capabilities and therefore inadequate sharing of information about the virus and its means of transmission, and customs regarding the treatment of dead bodies that can facilitate the spread of the virus. A recent report by Save the Children identified 28 countries with health systems that are equally or more vulnerable to Ebola than Liberia, which experienced the most deaths from the recent outbreak.[35]
2013 Outbreak and 2014 Transmission
Outbreak
In many ways EVD emerged in the perfect environment for an outbreak. Ground zero of the current epidemic in Guinea, Liberia, and Sierra Leone was a village near Gueckedou, Guinea, at the convergence of the three countries’ borders. The region is heavily forested and inhabited by a collection of ethnic groups, which span all three countries and communicate via a common trading language—Malinke (also known as Mande and Mandingo). On the Guinea side, this is the only part of the Muslim majority country where Christians and Animists predominate, further minimizing the area’s political influence. While the three countries have different colonial traditions—British in Sierra Leone, French in Guinea, and freed American slaves in Liberia—the local populations are not troubled by official borders and routinely cross back and forth to trade and visit relatives.
This region in West Africa has suffered almost continuously from decades of simultaneous or sequential conflicts, often supported or instigated by one regime against another. Liberia went through several civil wars from 1980 to 2006. In Sierra Leone, conflict started in 1991 and continued until 2002. Guinea became embroiled in neighboring conflicts between 2000 and 2002, with internal political turmoil continuing until 2010. Even after hostilities ended, each country had to deal with the thousands who had been physically and emotionally traumatized and with the rehabilitation and reintegration of combatants and victims into society. Throughout these troubled decades, each country hosted hundreds of thousands of refugees. These conflicts gravely degraded the minimal infrastructure and government services that had existed, chased most professionals out of the countries, and created a general sense of distrust and cynicism among the people toward governing bodies. Officials are generally seen as corrupt, abusive, and self-serving. As a result, government pronouncements by the affected countries about EVD have been met with skepticism and disbelief.[36]
Observations. The three governments lack the resources and capacity to respond in any significant way to a major emergency. These countries possessed little semblance of a national health system before the outbreak, depending instead on a patchwork network of international NGOs such as MSF, missionary medical groups, and ad hoc support from WHO, the CDC, and other developed-world institutions. While such organizations are dedicated and professionally competent, they were never meant to be a substitute for national health systems.
In the affected countries the government-run health facilities lack resources, suffer from diminished sanitation conditions, lack running water, and face perpetual shortages of medical supplies and medical personnel. Families often must pay a bribe for patients to be admitted and examined. Family members are often responsible for feeding the patient, providing their bedding, purchasing the needed medicine, and caring for the patients’ personal hygiene. While urban physician-to-patient ratios may fare better, rural areas are often limited to one physician per 100,000 people.
In addition to poor public health infrastructure and trained medical professionals, an Ebola vaccine remains elusive, despite experimental success. Experimental treatments and vaccines are under development, but none have been fully tested and approved for commercial use. Since all previous outbreaks were small and localized, there has not been the demand for drugs or vaccines to incentivize pharmaceutical companies or others to invest in a vaccine. In 2005, however, scientists published the results of a trial vaccine, which was 100 percent effective in protecting monkeys from Ebola.[37] Despite these results, the vaccine was not tested further.[38] The extent and scope of the current outbreak have renewed interest in the stalled vaccine and other treatments. The WHO determined that it was ethical to bypass usual procedures and use experimental vaccines and treatment drugs to respond to the current outbreak. However, concerns remain about the effectiveness of clinical trials in West African countries with overwhelmed health care systems. Indeed, several infected American health workers returned home to receive treatment with experimental drugs including Zmapp. Yet attributing their recovery to experimental treatments remains difficult.[39]
Another potential treatment method is convalescent therapy, which involves giving current patients the blood of Ebola survivors, which contains antibodies against the disease that prevent further infection or spread of the virus to others. For example, the Bill and Melinda Gates Foundation sent three specially equipped bloodmobiles to collect purified blood liquid (i.e., plasma or serum) while allowing the patients to keep their blood cells. Researchers are still trying to determine which antibodies they need to collect, the needed concentration, and which groups might be willing to donate serum under what conditions.[40] WHO is also considering using gene therapy,[41] and other scientists are studying how people infected with EVD in earlier outbreaks, especially the most recent one in Uganda in 2000, managed to survive and develop a strong immunity to the infection. The full testing process could take years to yield useful results.[42]
Even if some or all of these treatments are approved, payment and access will pose problems. Furthermore, the virus evolves quickly, making it unclear whether a successful vaccine or drug treatment would protect against future outbreaks.[43] However, research has shown that survivors appear to be resistant to the particular strain of the Ebola virus that they contracted, suggesting a reduced likelihood of repeated infection. Blood samples taken from Ebola survivors a few years after infection show that they developed antibodies capable of neutralizing the virus.[44] Aid agencies hire these survivors as health workers to help care for those infected.[45]
Findings. With the EVD outbreak, what little health care infrastructure that existed in Western Africa rapidly collapsed. Doctors and nurses left hospitals, administration ceased, and clinics and other medical facilities closed. While the world’s attention is focused on EVD, the erosion of health services impedes treatment of day-to-day ailments and diseases, which have great incidence and prevalence. Patients cannot get vital anti-malarial drugs, and mothers lack prenatal and postnatal care. Routine medical issues result in increased preventable deaths—more than those from EVD.
While some measure of normalcy is expected to return to the health care systems within the affected countries after the EVD outbreak is contained, whether the countries will improve the capacity of their health care systems after the crisis remains to be seen. Improvement is critical to stopping future outbreaks of EVD or other viruses from becoming regional epidemics or established endemic diseases. Additionally, the economic downturn resulting from the EVD outbreak will only exacerbate the inherent weaknesses of the health care infrastructure in these countries.
The World Bank has estimated that Guinea, Liberia, and Sierra Leone will lose at least $1.6 billion in economic growth in 2015, while further economic analysis has determined that Sub-Saharan Africa could lose ranging from a conservative figure of $500 million to a high of $6.2 billion.[46] These large figures account for all types of economic losses, including trade and commercial activity, foreign investment, and tourism. Yet improved health care services in these countries are critical for stability and economic recovery.
Strengthening the health care infrastructure will not only help the local populations, but also encourage international investment to return, helping to further mitigate longer-term economic damage.
Recommendations. A robust, multipronged, and coordinated global response is crucial to addressing the current crisis, strengthening the health care infrastructure, preparing for future outbreaks, and mitigating widespread economic devastation. The immediate priority is containment. International organizations, NGOs, governments, and the private sector must be included in the response to a crisis of this magnitude because no one organization has the capability to address the crisis fully by itself. To recover from the outbreak, the international community should:
- Identify a lead coordinating body at the outbreak stage—ideally a reformed WHO. As WHO Director-General Dr. Margaret Chan admitted, “This was West Africa’s first experience with the virus, and it delivered some horrific shocks and surprises. The world, including WHO, was too slow to see what was unfolding before us. Ebola is a tragedy that has taught the world, including WHO, many lessons, also about how to prevent similar events in the future.”[47] While WHO is the most natural international coordinating body to lead the response to an outbreak, it has demonstrated a troubling lack of initiative and decisiveness. This is due, in part, to structural and bureaucratic inefficiencies. However, WHO has also tended to focus on non-core initiatives, such as tobacco use and childhood obesity, that distract it from its correct focus: building the capacity of national health systems in developing countries and monitoring and coordinating the international response to epidemic disease.
- Develop sustainable and capable medical personnel pipelines in the affected countries and region. A system should be developed to incentivize doctors and nurses upon completing their education to stay and work in their home countries. Educational assistance programs, guaranteed placement, and other incentives could be implemented to encourage qualified personnel to remain in country.
- Strengthen overall hospital infrastructure management by developing reliable and resilient health care systems. EVD-affected countries should seek to establish partnerships with private health care companies to help to implement internationally recognized standard operating procedures. These procedures would improve both the quality and effectiveness of local care delivery networks and build a bulwark against future disease outbreaks.
- Continue vaccine development. While the number of EVD cases has decreased, the potential for a future outbreak remains high. Besides continued vaccine development, the international community, particularly governments in high-risk areas, should develop sustainable logistical chains, especially for personal protective equipment (PPE) and “cold” chain management for treatment, vaccines, and drugs.
- Engage the private sector to help to advance the development, expertise, and capacity of EVD-affected governments and those with vulnerable health systems. The private sector has proven experience in improving logistics, refining supply-chain management, bolstering client relations, and implementing data-driven solutions. The international community should leverage this expertise to develop long-term health care strategies to deal with primary care and emergency health care challenges, including EVD.
Transmission: Cultural and Societal Factors
Observations. Cultural factors compounded the outbreak. In rural areas there is a general belief that marabouts (witch doctors) can cast spells and possess medical powers, which are often trusted over proven international practices. In addition, bush meat—wild game from the forest, including fruit bats, which are believed to host the Ebola virus—is a highly popular delicacy and the preferred meat of choice, including in West African cities.
African burial rituals can also contribute to the spread of the disease. Some West Africans maintain the belief that the day you die is among the most important days of your life. Final farewells are usually a hands-on and affectionate ordeal as the body is often washed, dressed, and carried though the community. Friends and relatives sometimes even share a final drink with the deceased, putting the cup to the lips of the deceased before taking a drink themselves.[48] Kissing the body is also common. These practices can be extremely dangerous because Ebola victims are often most contagious just after death, when the viral load in their blood is at its highest. Furthermore, EVD can survive for several days on the skin of an infected body. The hemorrhagic aspect of Ebola can also lead to the emission of blood (and sweat) through the pores, creating a thin layer of highly contagious film covering the body.[49]
On the other side of the spectrum, in many cases those who become infected can be highly stigmatized, cast out of their communities, or left isolated in their homes without access to care. Fear of ostracism has led infected individuals to avoid hospitals and clinics at all costs. In Liberia, for example, there have been multiple reports of patients running away from clinics or avoiding transport to hospitals. For those who have had sick family members, but have been declared healthy, returning to everyday activities is often difficult because community members do not want them at work, in markets, or at places of worship for fear that they are also infected.
The epidemic has greatly affected children. According to the United Nations Children’s Fund (UNICEF), more than 16,000 children have lost one or both parents. Relatives often are too afraid to take them in as they usually would.[50] Fearful locals worry that curfews and quarantines will make them more susceptible to the disease. Countries recovering from recent civil wars are known for having increased distrust between governments and their people.[51] Compounding the mistrust is the fact that many health workers and security forces are foreigners who often do not speak the native language and are unaware of local customs. Rather than send loved ones away to clinics where visitations are limited, many families believe that they can give decent care in their own homes with the help of prayer and faith healers.[52]
Findings. A speedy, comprehensive, preplanned, flexible response coordinated among national and local governments, aid organizations, civil society, and the private sector can quickly mitigate Ebola’s spread.
EVD can spread exponentially, which makes a quick and comprehensive response critical to subduing an outbreak. A pre-existing plan facilitates timely treatment of victims and rapid tracing and monitoring of those who have been exposed to the virus. Public education enables people to protect themselves from infection and avoid confusion and fear. Every day that passes before the response is launched heightens the potential loss of life.
Effective coordination at all levels of government reduces the possibility of response gaps, which is particularly important during tracing and monitoring activities, which require meticulous, labor-intensive effort.
Private-sector for-profit and nonprofit organizations are important force multipliers that can often respond more nimbly and more precisely than a government can during a crisis. They often have deep local knowledge and have built trust with communities based on their pre-existing relationships. This knowledge and these relationships can facilitate the response, allowing delivery of aid to the neediest recipients.
Recommendations. The United States should maintain its leadership position in the efforts to fight EVD in West Africa. Recent experience has taught that, as long as the epidemic continues, transnational transmission is possible and the United States remains at risk. More help is needed to end the outbreak and transmission. On January 21, 2015, the U.N. declared that it needed an additional $1.5 billion in funding for the first six months of 2015, of which $500 million has been funded.[53] There are also critical shortfalls in other areas, particularly of trained medical personnel. The United States should lead the response by increasing its efforts to address these gaps. Specifically, the United States should:
- Redouble its efforts to gain commitments from those countries that have not significantly invested in the outbreak response;
- Continue support for technological innovations such as vaccine development, rapid-result Ebola testing, and mobile lab creation in preparation for future outbreaks; and
- Assist countries neighboring the affected West African countries in establishing humanitarian corridors to the affected countries.
Transmission: Global Network
Observations. International travel has emerged as one of the most contentious issues surrounding the Ebola virus, and countries are divided in their responses. Whereas health workers who knowingly have direct contact with Ebola patients are aware of the symptoms, asymptomatic foreign travelers may unknowingly carry the deadly disease to other countries. African countries were the first to institute travel bans, usually on travelers from Guinea, Sierra Leone, and Liberia. Many countries began symptom screening of passengers from West Africa, and some even banned flights from the region. Several states set up mandatory quarantines. Saudi Arabia banned people from Guinea, Sierra Leone, and Liberia from entering the country and denied visas for the hajj pilgrimage for fear of facilitating disease infection.[54] Even countries unlikely to be directly in the virus’s line of fire began to take precautions. For example, North Korea announced that it was closing its borders to foreign tourists regardless of country of origin beginning on October 24, 2014.[55]
WHO and other emergency experts have called travel bans counterproductive in fighting the spread of the virus. They have cited the low numbers of infections outside West Africa and warned that shutting down air travel in West Africa would only increase the region’s economic problems. They also worry that mandatory quarantines increase the stigma against survivors of Ebola or asymptomatic people from infected regions (“Fearbola”), deter vitally needed foreign health care workers from travelling to infected regions, and lead travelers to lie to evade the system, thus increasing the risk of further, unknown spread.[56]
The international health community, led by WHO and the CDC, attempted to balance these concerns with outbound travel measures meant to identify problematic travelers before they entered the international aviation network.[57] However, the delay between infection and the presentation of symptoms means that such screening is not foolproof. The fact that health systems in West Africa are significantly weaker than those in the more developed world may also create an incentive to travel for a person who believes he or she is infected.
Following weeks of deliberation after the crisis arose, the United States implemented specialized screening for international travelers with the goal of identifying possibly infected passengers. On October 8, 2014, DHS implemented new requirements funneling passengers from affected countries (Guinea, Liberia, and Sierra Leone) through five gateway airports—Kennedy International, Washington-Dulles, Newark Liberty, Chicago-O’Hare, and Hartsfield-Jackson Atlanta—with passengers receiving a medical review by Customs and Border Protection (CBP) and the CDC.[58] On January 6, 2015, DHS and the CDC ended a requirement implemented on November 16, 2014, for specialized screening of travelers arriving from Mali due to a lack of new cases, but the requirement remains for the original three countries.[59]
The calls in Congress to implement a visa and/or travel ban from affected countries died down to some extent after the implementation of the specialized screening.[60] However, whether such a ban can and should be part of an effective strategy against an infectious disease remains a question in hot debate.
Findings. In future responses to public health crises, epidemics, and pandemics, it is important to make clear that while there are tools for controlling movement across global networks, such measures have very limited impact on containing the problem, short of extreme policies of completely shutting down cross-border movements. In light of the nature of international travel, the limited ability to track the movement of people through the global transportation network, the difficulty of accurately screening for symptoms, and the length of any incubation period, resources would be best dedicated to containing the problem at the source through assistance, expertise, and resources on the ground. However, the movement of travelers through international transportation networks presents opportunities to screen for problematic individuals.
Recommendations. The United States should:
- Play a leadership role in organizations, such as the International Civil Aviation Organization and WHO, in developing safety standards and best practices that nations can implement quickly at their airports (and perhaps other ports of entry) to screen passengers in the most effective manner without disrupting legitimate travel;
- Work with allies to develop specialized procedures for medical personnel traveling to and from affected regions due to their higher likelihood of infection and the critical nature of their travel to combat disease on the ground;
- Encourage other countries to work with air carriers to implement advanced passenger information systems (APIS), allowing for faster, more complete contact and tracking in the event of an infected passenger; and
- In extreme situations, consider additional requirements in the visa application process, such as a delay in issuing the visa after the interview to ensure that individuals are not incentivized to attempt to travel if they believe they may have been exposed to an infectious disease.
International Response
Humanitarian Assistance for West Africa
Findings. Senegal and Nigeria responded quickly with a coordinated, massive effort involving the public and private sectors and using a pre-existing response plan. Their responses resulted in both countries being declared Ebola-free in relatively short order.
In August 2014, EVD reached Lagos, Nigeria’s largest city, brought by a traveler from Liberia. Once the index patient was diagnosed, Nigerian state and federal officials quickly acted, adapting a pre-existing contingency plan for a mass polio outbreak. An interagency Ebola operations center was established just three days after the first case was confirmed. Officials in the center worked with airlines, travel agencies, and hospital administrators to identify nearly 900 at-risk individuals who had contact with the index patient. These individuals were subject to a rigorous protocol, including twice daily in-person monitoring.
According to a CDC report, working outward from the initial list of at-risk individuals and eventually interviewing neighbors and others in close proximity to at-risk individuals, specially trained Nigerian case management personnel visited some 26,000 homes and conducted 18,500 face-to-face interviews over the following two months. Persons exhibiting Ebola-like symptoms or who were likely exposed to the virus were transported to suspected-case isolation wards at nearby hospitals by the monitors. Those who subsequently tested positive for EVD were moved to confirmed-case wards.
Nigerian authorities also embarked on a multimedia campaign to educate the public about the disease, using billboards, posters, television, and radio. Businesses and private groups also contributed to the efforts. One nonprofit research organization supplied health care workers with mobile phones and an app that eventually reduced the lag in reporting the onset of symptoms to almost real time. Another group of volunteers banded together to use Facebook, Twitter, and other social media to educate Nigerians. The group also partnered with the government to operate a telephone helpline. Ultimately, Nigeria’s population of more than 175 million people had only 20 confirmed Ebola cases, resulting in eight deaths.
Senegal’s response was similar. Months before diagnosis of its first and only case of EVD, Senegalese authorities had a detailed response plan in place, coordinated by the president’s office and involving multiple government agencies. In August, the first case was confirmed: a young man arriving from Guinea. Once the case was confirmed, 74 individuals who had come in contact with the patient were quickly identified and subject to close monitoring by government officials and twice daily checkups by medical personnel. Simultaneously, Senegal closed its 330-kilometer land border with Guinea and banned flights and ships from Guinea, Sierra Leone, and Liberia, while opening up a humanitarian corridor through its airport to facilitate the seamless movement of humanitarian personnel and supplies, subsequently becoming a key hub for assistance to the region.
Dr. Awa Coll-Seck, Senegal’s Minister of Health, told WHO officials that her country’s successful battle to contain the disease’s spread included an intentional policy of supporting “the reintegration of the recovered patient into a society that could understand why he posed no risk of contagion to others” as well as providing direct assistance in the form of money, food, and counseling to those in contact with the patient as a strong incentive for their cooperation.[61] In the end, Senegal’s single patient survived, and all those with whom he had contact completed the full three-week follow-up.
WHO’s failure to effectively address and respond to the initial EVD outbreak in West Africa likely hindered global response efforts and led to the disease spreading beyond Guinea. Given the region’s high concentration of deadly diseases, poor health care systems, and uneducated populations, WHO’s failure to acknowledge the seriousness of the outbreak, particularly once EVD reached highly concentrated urban areas, is deeply concerning.
The very entity responsible for monitoring and reporting such outbreaks was silent and, when forced to act, the agency proved woefully unprepared to coordinate the international community’s response. Luigi Mariano, Deputy Director of MSF Switzerland, observed in one news report:
In all the meetings I attended, even in Conakry, I never saw a representative of the WHO…. The coordination role that WHO should be playing, we just didn’t see it. I didn’t see it the first three weeks and we didn’t see it afterwards.[62]
While the initial outbreak began in December 2013, WHO waited until early August 2014 to declare the situation in West Africa an international health emergency. WHO Director-General Dr. Margaret Chan stated, “This is the largest, most severe, most complex outbreak in the nearly four-decade history of the disease.”[63] What remains clear to most observers is that the situation in West Africa could have been far smaller, less severe, and simpler to contain if WHO had acted sooner. MSF warned of the unprecedented scale of the outbreak as early as March 31, 2014.
While many governments in the region appeared to have been in denial during the early days—this was the first EVD epidemic in the region—WHO had a critical role of responding and alerting the international community of the situation if the health care systems and health infrastructure failed. Yet the international response was weak according to NGO officials. Dr. Bart Janssens, MSF’s Director of Operations, said that WHO “played a critical role in that failure in the first two to three months…. They were in the same mode of denial as the governments were.”[64] MSF President Joanne Liu declared that WHO failed its “mandate to help member states cope with health emergencies.”[65]
Observations. Some of WHO’s failings have been blamed on its regional system and political appointments. There was a lack of coordination between the Africa Regional Bureau and the headquarters in Geneva, a problem many have blamed on the local and international leadership. Ultimately, after coming under greater criticism, WHO headquarters took over responsibility for coordination in West Africa from the Africa Bureau. WHO also sent experienced staff to run country offices. Many argue this half measure was too little, too late. Dr. Peter Piot, a former WHO official and co-discoverer of Ebola, said the delay in direct leadership by Geneva “was a crucial factor in allowing the epidemic to reach unprecedented levels.”[66] Indeed, the government of Guinea took nearly three months to make its first official report of EVD to WHO. By that point, the disease was spreading. Yet WHO’s inability to get in front of the disease and provide the leadership necessary in this public health crisis highlights serious concerns over the agency, its structure, resource allocation, and priorities.
In light of WHO’s shortcomings in dealing with EVD, many of the criticisms (including an internal WHO memo[67]) blame politically driven appointments, bureaucracy, and a lack of disease monitoring. These are not new problems. Similar criticism was directed at WHO during the H1N1 (swine flu) outbreak in 2009.[68] Yet despite an external review investigation producing a list of needed reforms, the problems persist. As recently as January 2015, Margaret Chan blamed inadequate WHO funding for WHO’s failure to respond to the EVD outbreak early. She called for a “dedicated contingency fund to support rapid responses to outbreaks and emergencies”[69] rather than advocating for smartly and effectively allocating resources to priority public health emergencies. Instead of focusing on WHO core areas, such as deadly infectious diseases, the agency diverts scarce resources to noncritical issues, such as childhood obesity.
Recommendations. The WHO member countries need to have a serious discussion about WHO’s future, not only examining what went wrong during the EVD outbreak, but also investigating more deeply into why the agency continues to fumble in potentially catastrophic public health situations. If Ebola had started in a deeply connected corner of the world, the story could have unfolded very differently.
Specifically, WHO member countries should:
- Narrow the organization’s priorities to focus on a limited number of core responsibilities: building national health capacity, monitoring and tracking disease outbreaks, developing national and regional outbreak response plans, coordinating and managing rapid deployment commitments, and encouraging development, especially by promoting the protection of intellectual property, vaccinations for neglected diseases, and new antibiotics and treatments as resistance rises;
- Emphasize and encourage multilateral and bilateral health funding and building public health expertise and capacity in developing nations; and
- Strengthen lines of authority and responsibility in WHO to avoid repetition of the politicization and inefficiencies that slowed WHO’s Ebola response and exacerbated the situation.
Efficient Trade Rules for West Africa
Much of the discussion on combating the Ebola epidemic has focused on immediate solutions to slow the outbreak and limit its damage. However, long-term barriers will continue to inhibit effective response to future public health emergencies. Perhaps the most important tool in combatting EVD is ensuring that the proper supplies, medications, and equipment reach health care workers in the affected countries. Since most of these supplies are transported internationally, supply chains must be developed to procure equipment. While organizations such as WHO, the U.N., and the U.S. military have set up supply chains for medical equipment in the short term, inefficient and costly local customs, procedures, and regulations may hinder long-term solutions. Barriers to international trade, particularly customs delays, may slow future responses to epidemics by limiting the availability and accessibility of medical supplies.
Observations. With small and poorly developed domestic markets, EVD-affected economies—such as Guinea, Liberia, and Sierra Leone—must rely on international markets for medical supplies and pharmaceuticals. Most supplies are imported by air freight or commercial shipping. However, customs and regulatory delays in affected countries have historically impeded access to these markets and damaged local supply chains. These impediments fragment supply chains and render them unreliable and unpredictable, threatening the delivery of vital medical supplies.
When goods arrive at West African airports and seaports, they must clear customs before moving on to their final destination. However, these goods often sit idle as administrative forms are processed and duties paid. According to the World Bank, once a container arrives in Guinea, Liberia, or Sierra Leone, it requires an average of nine documents, 29 days, and $1,458 to deliver it to its destination. These complications increase the cost of importing, unnecessarily delay shipments, and divert resources to document compliance.
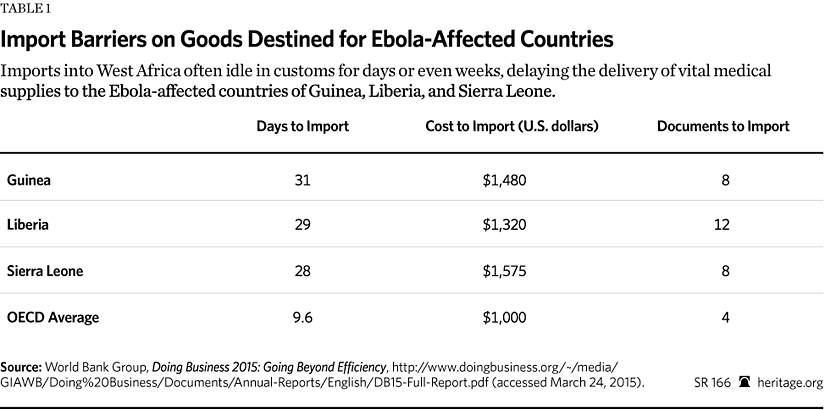
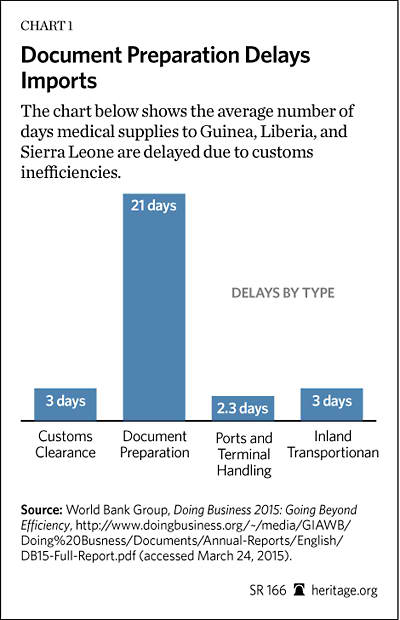
In particular, customs clearance forms and other documentation translate directly into delays. Containers take nearly a month to reach their destination after arriving in country as companies and government administrators struggle to process the paperwork and ensure burdensome regulations are followed. In Guinea, Liberia, and Sierra Leone, completing the required documents can take up to three weeks after goods have arrived in country.[70]
These delays threaten the timely delivery of pharmaceutical supplies and upset logistics chains and business inventories that rely on timely shipments. According to a report by the University of Westminster, local logistics managers in Sub-Saharan Africa report that inventory management, transportation, and distribution are the greatest challenges to medical supply chains on the continent. Procedures that delay medical supplies in clearing customs disrupt supply chains and introduce uncertainty into the process.[71]
Such delays pose an even greater threat to sensitive products that must be refrigerated during shipping, such as vaccines and other medicines. These goods are often “time sensitive and more subject to inspection” than regular goods, threatening the development of reliable international “cold chains” that can deliver critical medicines in good condition.[72] Delays at border crossings and customs clearing areas can harm or destroy expensive vaccines and other medicines bound for infected individuals.
Findings. Customs delays, particularly in documentation, impede medical supply chains in Ebola-affected countries. Currently, government task forces in Guinea, Liberia, and Sierra Leone are helping to expedite customs clearance for Ebola-related goods. These include partial waivers for clearing goods and fast-tracking documents and duty waivers. In some cases, this has reduced import time to between 24 and 72 hours. However, these emergency government task forces are not long-term solutions for efficiently importing medical and pharmaceutical goods in the future.[73] To respond quickly to unfolding crises, officials must be able to rely on pre-existing infrastructure while additional resources are mobilized. If regulations and administrative delays hinder the development of this infrastructure for medical supply chains, governments and public health officials will have more difficulty controlling future outbreaks.
Recommendations. To facilitate creation of efficient distribution channels that deliver products on time and in a useable condition, national governments in the region should improve customs procedures and embrace trade freedom. Specifically, they should:
- Reduce delays by cutting documentation. Aside from cost, import documentation is the largest impediment for importers in all three countries. Governments should work to cut documentation and align regulations and automation procedures with global standards.
- Permanently institute customs fast tracking and duty waivers for medical goods. Affected countries should use fast-tracking procedures, even after current emergency task forces are dissolved.
- Speed up Liberia’s World Trade Organization (WTO) accession timeline. Liberia can do this by submitting an application without delay and by resolving any long-standing issues with WTO members. Accession into the WTO will lower tariff rates and improve harmonization and automation of customs procedures.
Long-Term Impacts and Economic Stability
President Barack Obama has declared that containing the Ebola outbreak is a top national security issue, and U.S. investments of money, military personnel, and health care professionals have established the U.S. as the leader of the international response to the epidemic. Yet the U.S. still needs to address the significant short-term, medium-term, and long-term impacts of the epidemic.
Observations. Guinea, Sierra Leone, and Liberia have suffered severe economic and social damage. They were already near the bottom of the U.N. Development Program’s Human Development Index before the Ebola outbreak, and the World Bank has dramatically downgraded projected economic growth for these countries because of the outbreak. Sierra Leone’s economy was originally projected to grow by more than 11 percent in 2014, but the World Bank estimates it grew only 4 percent. Liberia’s growth was estimated to reach 6 percent, but is now estimated at less than half that. Guinea’s expected economic growth rate was around 4.5 percent, but is now believed to be approximately 0.5 percent. These downturns are a major blow for the affected governments, and the projections for 2015 are equally grim. The World Bank estimates that economic losses in Sub-Saharan Africa could reach $6.2 billion.[74]
In the medium term, companies are retreating. Liberia’s two biggest investors in the mining sector have essentially ceased production, and 46 percent of Liberians employed before the crisis are no longer working. Employment losses have made it harder for people to afford soaring food prices resulting from decreased agricultural output. The U.N. estimated that, barring significant intervention, more than 1 million people in these three countries would experience food insecurity by March 2015.[75]
The social damage is severe as well. Liberia and Sierra Leone were recovering from decade-long civil wars that tore them apart, devastated their economies and basic infrastructure, and led to major population losses. The Ebola crisis stressed already weak health, commercial, and other social infrastructure, further damaging the social fabric of these countries.
Furthermore, Ebola has orphaned an estimated 16,000 children. Many schools were shuttered for months and have only recently begun reopening. Seventy-five percent of EVD victims were women, who have been more vulnerable because of their traditional caregiving role. As of January 21, 2015, 499 health care workers had died from Ebola in the three countries, causing some clinics to close entirely.
Findings. The economic and social losses from the outbreak profoundly threaten the stability of the affected countries and the region. The reduced economic growth from an already low base will significantly affect the ordinary people suffering from the health crisis. The loss of revenue means that governments will continue to struggle to deliver services to their people after the outbreak is over and make rebuilding even harder. Furthermore, the countries will have difficulty creating new jobs and replacing the workers who were lost to the epidemic.
The crippling blows dealt to the already weak health care systems will make them dangerously inadequate to treating populations, which have some of the lowest life expectancies in the world. Additionally, thousands of children whose education was disrupted will be less equipped to rebuild their countries.
Poor harvests are expected in 2015 due to the epidemic disrupting the 2014 planting season, deepening the looming food crisis. In normal years, about 45 percent of the population in Sierra Leone cannot obtain adequate food from June to August. Barring intervention, that percentage will certainly rise, and the hunger will become more acute.
The epidemic has also damaged the basic trust between peoples and communities, which is necessary for functioning economies and governments, leaving these countries vulnerable to unrest and violence for the foreseeable future.
Recommendations. The USG should continue to work to ameliorate the dangerous long-term effects of the epidemic. The recovery and long-term health of the hardest-hit countries will require a sustained commitment from the United States and the rest of the international community. The United States and the international community should:
- Provide short-term funding to the affected countries to bolster budgets drained by revenue loss and increased expenditures;
- Encourage economic growth by promoting trade with and private-sector investment in the affected countries; and
- Help affected countries establish reintegration programs for EVD survivors and incentive programs to encourage cooperation from people who will be in contact with the recovered patients.
U.S. Government Response in West Africa
Observations. On September 16, 2014, the White House released a statement describing the Ebola epidemic in West Africa as a national security threat to the United States. In the statement, President Obama announced that a bipartisan consensus approving U.S. involvement existed and that both pragmatic and moral considerations required the U.S. to lead the international effort to counter EVD in West Africa.[76] Although the United States never banned travel to or from West Africa, since October 22, people entering the United States from the region have been subject to enhanced monitoring during their first 21 days in the United States.[77]
In response to the epidemic, the USG deployed some 3,000 troops to West Africa in September 2014. These troops provided emergency assistance, including transporting supplies to remote locations and building EVD treatment units. In many aspects the U.S. military was the face of the U.S. response to the EVD outbreak in West Africa, but it was not the primary organization leading U.S.-sponsored relief efforts in the nations affected by Ebola. Rather, the U.S. military—specifically, the U.S. Army, Air Force (USAF), and Marine Corps (USMC)—played a secondary role, supporting the United States Agency for International Development (USAID), which was the lead U.S. agency.[78] Furthermore, the Army was the lead military agency operating in the Ebola-affected countries, primarily Liberia, with the USAF and the USMC acting in support.
While the close relationship of the Department of State, USAID, and U.S. Africa Command (AFRICOM) is largely uncharacteristic in the other combatant commands and has been the subject of criticism in the past, it served as a point of strength and proved to be an asset in responding to the EVD outbreak. In the current outbreak, the relationships and institutional knowledge maintained by all three organizations proved to be quite useful, serving as the key driver of a quick and effective response.
The military forces deployed in response to the EVD outbreak were not troops specially designated for pandemic and humanitarian relief services. Rather, they were conventional forces used for their designated skills to assist in humanitarian efforts under the direction of USAID. Furthermore, the troops sent to West Africa as part of the U.S. response were deployed over a vast geographical area. For example, one contingent of airmen was spread over three geographically detached areas: Liberia, North Africa, and Iraq.[79]
Although the U.S. military is unmatched in capability and capacity, challenges were still present in the U.S. military’s coordinated response to the EVD outbreak in West Africa. Specifically, while the U.S. has tremendous expeditionary capabilities that enable it to put forces on the ground in a remarkable time frame, some impediments challenged the services’ ability to accomplish their mission. These impediments included weather (and its effect on the terrain) and the wide dispersal of the forces operating in the region.
In response to the EVD outbreak in West Africa, the U.S. was fortunate to have partner host nations in the region, where forces could assemble and store supplies before final shipment to the Ebola-affected countries. These regional partners also accommodated troop movements—including basing, overflight, permission to launch and return, and personnel monitoring—which were critical for U.S. troops leaving for and arriving from Ebola-affected countries.
Findings. Through multilateral institutions and bilateral aid, the USG has contributed hundreds of millions of dollars in humanitarian aid, PPEs, water treatment units, disinfectant, and other basic supplies for affected countries. As of February 11, 2015, the USG had provided more than $963 million in assistance to West Africa for EVD outbreak response. This includes humanitarian assistance funding distributed to USAID, the Department of Defense (DOD), and the CDC.[80]
The U.S. military faced a series of challenges in executing that mission that they were not specifically trained to handle. Shuffling troops across diverse and detached geographic areas also posed additional problems. While these difficulties strained the military’s limited resources and personnel, U.S. troops performed well and accomplished the directives laid out by USAID. This can be attributed to the unique relationship that AFRICOM maintains with its civilian counterparts.
The speed and flexibility of the military deployment to West Africa showcased the expeditionary capabilities required to complete this type of emergency humanitarian operation effectively and successfully. Military personnel who participated in the operation have stressed the importance of airborne lift. They claimed it was an advantageous capability and that they could not have executed their mission as planned without it. Citing the particularly wet season in Liberia as an unexpected impediment, military officers stated that systems such as the MV-22B Osprey (a tilt-rotor vertical takeoff aircraft) allowed them to deliver critical lifesaving supplies in areas where the roads were significantly degraded by severe rain.
Recommendations. The U.S. should:
- Constantly examine and reassess its force posture. The EVD outbreak in West Africa demonstrated that the international community cannot predict where the next epidemic will originate. Forces dedicated to a specific area of operations would allow for a dedicated, measured, and deliberate response. While U.S. forces overcame being geographically dispersed, maintaining a high level of readiness after traveling a long distance is taxing on troops. For example, the flight to West Africa from Moron, Spain (where the Special Purpose Marine Air-Ground Task Force Crisis Response Africa is based) is comparable to the flight from Washington, DC, to Moron, Spain.[81] Maintaining a unit’s full resources in one designated area of operations provides the troops participating in the mission with maximum access to the tools that they need to be successful.
- Continue to fully fund the DOD to ensure continued research and development in flexible, next-generation transportation platforms. As the wet weather season in West Africa demonstrated, especially in Liberia, the services need flexible systems that enable them to accomplish the mission regardless of the elements.
- Consider launching operations from sea in response to future epidemic-related humanitarian relief crises. Sea-launched (carrier-based) operations would provide U.S. forces with greater flexibility and would eliminate many contentious issues that could arise, such as procuring basing and travel permission from host countries. While U.S. forces secured agreeable terms with the host nations, this is not guaranteed in future crises. Colonel Robert Fulford, commander of Marine units deployed in AFRICOM’s Operation Unified Assistance, has stated, “We have great partners in the host nations…but it’s not a guarantee that they’re always going to allow us to go; it’s also not a guarantee that they’re going to allow us to come back after the mission.”[82] Additionally, enhanced maneuverability would give local commanders the ability to strategically position troops, which could support missions at the operational and tactical levels.
Domestic Response in the U.S.
Public Health and Medical Response
Observations. The United States was unprepared for a few cases of EVD, much less a major public health threat such as bioterrorism or a virulent pandemic influenza. A number of examples from the Ebola response highlight shortcomings in the nation’s programs intended to ensure preparedness for a public health crisis. These have ranged from a failure to properly identify suspected patients to a serious accident at the CDC’s main research laboratories.
The Dallas hospital that cared for Thomas Eric Duncan is a sophisticated medical center, but failed on a number of fronts. It initially misdiagnosed him and sent him home where he could potentially infect others. The hospital also failed to prevent the Ebola virus from spreading to its workforce, with two health care workers becoming infected with EVD.
Findings. Health care workers in the United States lacked the necessary training, equipment, and experience to protect themselves against biological agents and pathogens of this kind. State leaders exacerbated the problem by providing conflicting guidance. For example, the governors of New York and New Jersey issued quarantine orders, but others did not, leading to confusion about quarantine rules and standards.
The CDC issued guidelines that were ambiguous and did not pass the “common sense” test. Health care workers who had treated symptomatic Ebola-infected patients were not classified as being at greater threat than individuals who had not been exposed or in contact with infected patients. Likewise, the CDC belatedly identified and prepared the hospitals best suited to care for Ebola victims.
The Ebola crisis demonstrated that there is no such thing as “just-in-time preparedness.” Instead, preparedness activities need to be interwoven into the health care system to ensure that hospitals are prepared to confront the challenges they face. Of the $2.8 trillion spent annually on the health care system, only $250 million is directed to hospital preparedness. This is less than 0.01 percent of total expenditures. The current approach to reimbursement and funding considers public health and medical preparedness separate and distinct from routine health care when in fact it is not.
The nation lacks effective medical countermeasures—including therapeutics, vaccines, and diagnostics—for many public health threats. There is no commercial interest in many of these because developing them can take up to 10 years and $1 billion each, and then there may be no commercial market. This is compounded by current federal investments, which are insufficient and unbalanced. While pharmaceutical companies invest approximately 45 percent of their funding into basic research and 55 percent in advanced development, HHS invests 80 percent in basic research ($1.6 billion at the National Institute of Allergy and Infectious Diseases) and only $415 million in advanced development.
Clinical trials for countermeasures are also falling behind. For example, while the National Institutes of Health (NIH) announced a promising monkey trial for an Ebola vaccine in 2000, there is still no vaccine available today, more than a decade later.[83] This reflects both the lack of priority and resources for these kinds of countermeasures.
While the Food and Drug Administration (FDA) has demonstrated flexibility in rapidly responding to requirements for Ebola medical countermeasures, it has been slow to approve new medications—a process that must improve if new medicines are to make it to market. The agency should be prepared to change its standard processes during a public health crisis, recognizing the mortal threat that diseases such as Ebola pose.[84] The FDA has had some success fulfilling Ebola medical countermeasures requirements because much of the basic science and advance development research has been underway for a decade with funding for defense against bioterrorism. This is an example of the dual benefit of spending on biodefense: Improvements in rapid diagnostics, the ability to produce vaccines and therapeutics faster and less expensively, and improved capacity for surge medical care are good for defense against bioterrorists and naturally occurring diseases.
Recommendations. The U.S. government should:
- Identify medical facilities with expertise in particular infectious diseases and designate them as first-resort treatment facilities for victims. These facilities should be distributed throughout the country, equipped with containment and treatment units, and staffed with appropriately trained personnel.
- Integrate preparedness throughout federal, state, and local public health agencies. Just as the DOD emphasized jointness in its 1986 Goldwater–Nichols reorganization, the public health community should refocus on integrated preparedness. This would involve working with the stakeholder departments—including HHS, the Department of Veterans Affairs, DOD, and DHS—and state and local agencies to define joint requirements and develop comprehensive solutions.
- Integrate preparedness incentives into policy. Future health care reform efforts should consider incentives to enhance preparedness in the health care system.
- Expedite the approval processes for new medical countermeasures, including therapeutics, vaccines, and diagnostics.
- Adequately fund research and development of medical countermeasures. Erratic funding has caused serious delays in many programs critical to biodefense. Medical countermeasures are similar to sophisticated weapon systems in that they have very long lead times for development and deployment. Therefore, investments in medical countermeasures must be made years before the outbreak or pandemic, not during it.
- Invest in the capability to rapidly produce medical countermeasures in a crisis. Even if one of the EVD cure candidates currently in testing proves to be a “silver bullet,” America does not have the capacity to rapidly produce it in significant quantities. The 2012 establishment of the Centers for Innovation in Advanced Development and Manufacturing was a step in the right direction, but greater capacity is needed. In the 21st century, America’s pharmaceutical and biotech industries are part of the U.S. defense industrial base.
- In collaboration with all relevant parties, create uniform protocols for identifying, isolating, and treating victims and monitoring people exposed to the virus. Federal, state, and local governments and the relevant elements of the private sector should adhere to these protocols. When the various levels of government have different protocols, they breed confusion and inconsistent care and prevention. Standardization is needed across the spectrum.
- Partner with the private sector. The government should partner with private organizations and coordinate their activities to best use and leverage the expertise and knowledge of each to ensure an enhanced and cohesive national solution.
Federal Leadership
Observations. Senior Obama Administration leaders were not publicly or effectively engaged in the response. As the situation escalated, the Administration did not demonstrate visible, effective leadership. The Administration continued to treat the situation as a series of isolated medical incidents, rather than as the expanding regional and potential international outbreak that it was quickly becoming.
The Administration made CDC Director Dr. Tom Frieden the face of the Ebola response. While Dr. Frieden and the CDC played an important role in the medical response to the crisis, they lacked the stature, tools, and authorities necessary to coordinate the response effectively. The CDC is just one component of HHS, which is led by a Cabinet secretary and includes other relevant organizations, such as the NIH and the Office of the Assistant Secretary for Preparedness and Response (ASPR). Yet most HHS leaders were largely absent from public view, particularly those with statutory responsibilities.
Additionally, while HHS is certainly an important player in the federal government’s response efforts, it is one among the many departments with roles in the crisis. For example, DHS is responsible for border screening and DOD provides support to backstop the civilian agencies. The CDC has no ability to direct HHS or the response efforts of other departments.
Later, the President named an Ebola Czar—Ron Klain, a political operative with little discernible public health experience—to manage the interagency effort at the White House. He assumed the role at the White House from Lisa Monaco, the President’s adviser on homeland security and counterterrorism. Klain reported to Monaco and was not publicly engaged.
Findings. Agencies other than the CDC, with the appropriate statutory authority, could have been tapped to interface with the public. Following the slow, confused, and inefficient response to Hurricane Katrina, Congress passed the Pandemic and All Hazards Preparedness Act that created the position of the ASPR in HHS. As a result, the ASPR has a statutory basis to coordinate the public health and medical response to natural disasters in the United States during a declared emergency. The ASPR’s role extends beyond the CDC’s responsibilities to coordinating response efforts within HHS and throughout the federal government. Yet in the Ebola response, the ASPR was invisible.[85]
HHS Secretary Sylvia Burwell and DHS Secretary Jeh Johnson should have been more publicly engaged as their departments grappled with the escalating crisis. Indeed, HHS is to coordinate the federal response to health and medical incidents,[86] and the DHS Secretary is to be the principal federal official for domestic incidents.[87] In contrast, during significant terrorism threats during the Bush Administration, Cabinet officials were actively engaged in managing the situation. For example, Homeland Security Secretary Tom Ridge and Attorney General John Ashcroft held a number of joint press conferences explaining both the threats and the federal government’s actions to confront them.
Rather than bringing in a non-expert from outside government to manage interagency policy issues, the President should have called on experts inside the White House. Regrettably, the White House reorganization at the beginning of the Obama Administration eliminated the Homeland Security Council Biodefense Directorate, an office consisting of a Special Assistant to the President and a staff of physicians and public health officials. This office had successfully managed public health preparedness policy matters in the Bush Administration and provided expert advice to the President’s homeland security and counterterrorism adviser. A similar office and position also existed during the Clinton Administration.
Recommendations. The U.S. government should:
- Review the roles and responsibilities of DHS and HHS leaders during a public health emergency and ensure that efforts are appropriately coordinated. Homeland Security Presidential Directive 5 assigns the Secretary of Homeland Security the role of principal federal official for domestic incident management. The National Response Framework confirms this overall role for DHS and identifies HHS as the primary agency for public health and medical services. However, during the Ebola outbreak DHS and HHS leaders were largely absent from public eye, and it is unclear whether they played any leadership role during the crisis.
- Reestablish a White House office focused on public health preparedness policy akin to the Homeland Security Council Biodefense Directorate that existed during the Bush Administration.
- Resolve the role of the HHS Office of the ASPR, consistent with the intent of the Pandemic and All Hazards Preparedness Act.
Risk Communications
Observations. Government communication lacked risk messaging about the Ebola epidemic. Time and time again, communications literature shows that the public does not “panic” when confronted with information about a crisis. People do, however, want to know how the event (i.e., Ebola) will directly affect them. The 2014 Ebola epidemic showcased a lack of effective messaging, which left the public unnecessarily concerned.
The CDC announced the nation’s first Ebola case on September 30. The director emphasized that the patient would be isolated and that persons who encountered the patient would be contacted. However, additional information describing the technical risk of Ebola could have alleviated growing fear.
Instead of describing the nominal chance of contracting EVD, messages emphasized how current health systems and protocol would ensure public safety. Considering trust in all branches of the federal government is at or near a record low, messages about the government’s ability to mitigate the crisis would likely not resonate well with the public.[88] In general, social media on behalf of the White House and CDC did not adequately address the public’s need for information.
Findings. Communication about the news of the first EVD case in the United States should have included rational and evidence-based information about the virus to the public. Messages of assurance, certainty, and confidence in the current preparedness systems will not be helpful to those who remain skeptical of government and/or lack a background in public health or medicine.
Risk communication should acknowledge the public’s concerns. Acknowledging concern occurs when dialogue between responders and those affected by an event exists. The CDC Director attempted such a dialogue via a one-hour chat event during which individuals were invited to discuss the Ebola outbreak via Twitter (using #CDCChat).[89] However, the CDC lost control of the dialogue with many individuals tweeting questions outside the one hour allotted for the chat, and the designated hashtag was used for parody memes and information unrelated to the Ebola outbreak. In addition to their Twitter response, the CDC encountered challenges on Instagram. During the height of public concern, Instagram users left messages on CDC posts that were unrelated to the Ebola outbreak (e.g., smoking deaths). For example, messages demanded the agency “TALK ABOUT EBOLA,” and “post Ebola facts please.”
If the public believes their risk for contracting EVD is high, their expectations are built on this belief. If actions do not adequately address significant risks, communicators can perpetuate outrage toward the issue. For example, the White House explanation of the decision not to implement a travel ban was ineffective in resolving the concerns of the nearly two-thirds of the U.S. population who supported a ban on travel from Ebola-affected nations.[90] Due to the public’s ideologies and the belief that a travel ban could prevent Ebola from spreading in America, public outcry and subsequent political actions followed Obama’s announcement not to impose a ban. Public outrage, like in this example, is counterproductive to risk communication during a health crisis.
Communication should always acknowledge a certain level of uncertainty in messaging. For example, when the CDC announced that the Ebola virus could survive for several hours on surfaces like doorknobs and countertops, the social media response suggested that the CDC had been lying all along due to the fact that they had persistently stated that Ebola could only be spread by contact with bodily fluids. This sudden addition of new ways to contract Ebola only furthered the public’s distrust and fear of government entities.[91] Relaying certainty too soon can diminish trust, if progress toward containing Ebola slows or regresses, and it may prematurely communicate the end of the epidemic.
Conversely, Ron Dittemore, Program Manager NASA Space Shuttle, set the example for senior government leaders to follow on February 1, 2003. During the first press conference after the breakup of the space shuttle Columbia during reentry, he said:
As difficult as this is for us to do, we wanted to meet with you and be as fair and open with you, given the facts as we understand them today. We will certainly be learning more as we go through the coming hours, days and weeks. We’ll tell you as much as we know. We’ll be as honest as we can with you. And certainly we’ll try to fill in the blanks over the coming days and weeks.[92]
Finally, when assessing the fewer than 100 Ebola-related tweets posted by the CDC and the White House, an even smaller number of those messages actually provided instructional information—a staple in risk communication. With many messages bolstering the adequacy of the government to handle this situation, the involvement of government entities in ending Ebola abroad, or retweets from news sources, members of the public needed to seek out messages regarding specific details and instructional information on the virus. While the CDC and the White House provided links in their messages to subsequent information and those websites appeared to keep jargon to a minimum, no overarching strategy seemed to guide the response.
Recommendations. The U.S. government should:
- Increase collaboration across government to ensure that agencies and appointed officials are speaking with one voice. It is important to avoid conflicting or misleading messaging.
- Relay messages of technical risk. Communication should be specific in providing instructional information.
- Engage in a two-way dialogue with those affected by the risk and acknowledge public concerns.
- Improve messaging and acknowledge uncertainty. Leaders need to be open and honest with the American public. It would have been helpful if federal, state, and local political and public health leaders had said that there would be a learning curve as they dealt with this new threat—as during the severe acute respiratory syndrome (SARS) epidemic of 2003.
- Minimize unnecessary and unfounded certainty. Officials should not oversell or undersell the situation.
- Use social media effectively by preparing messages that apply these recommendations. Officials should be prepared to respond to emerging trends and social media needs.
The bottom line is that during the past 30 years, at least a dozen newly emerging diseases have come to America each decade. As the world becomes more crowded and jet travel makes it smaller, diseases will likely reach American shores with increasing frequency.
Incorporating Lessons Learned
Observations. Often lessons are observed, rather than truly learned. Despite a decade of planning and exercising, little evidence suggests that past lessons were incorporated into the Ebola response.
Findings. The DHS National Exercise Program (NEP) includes full-scale exercises involving top officials aimed at testing key vulnerabilities in America’s preparation, response, and recovery to a catastrophic event.
Although the program’s initial emphasis was to prepare for terrorist attacks, DHS recognized that other events could have large impacts across America. One of those events could be a biological event akin to the Pandemic Influenza of 1918. In 2005, the TOPOFF (Top Officials) III exercise used a pneumonic plague release in New Jersey to test several issues:
- Whether to quarantine people and shut down travel systems to contain the spread of the virus as transportation networks became compromised;
- How to communicate effectively between and among all levels of government and the public to keep first responders and the public informed and calm; and
- The capabilities of hospitals and the U.S. health care system to deal with a new and potentially deadly threat.
Following TOPOFF III, President Bush issued the National Strategy for Pandemic Influenza. The plan listed three pillars: preparedness and communication, surveillance and detection, and response and containment.[93] A May 2006 implementation plan highlighted “more than 300 critical actions…to address the threat of pandemic influenza.”[94]
Officials involved in TOPOFF III and the pandemic influenza strategy development effort spent time wrestling with the issues of travel restrictions, quarantining people, and other border control measures, communication among government entities and the public, and the resiliency of the health care system.
Despite this work nearly a decade ago, the response to the Ebola virus in the first several weeks appeared as if none of these exercises had occurred. From the inability to communicate a coherent message to the public to the inconsistent policy pronouncements on border control and containment strategy to the health care system’s failure to protect its own workers, the Ebola response fell short.
Just as New York City was lucky that the Times Square bomb did not detonate, the U.S. is lucky that it was an outbreak of the Ebola virus and not a more communicable virus like pneumonic plague.
Recommendations. The U.S. government should:
- Review lessons from the Ebola response and issue a public report, similar to the Bush Administration’s report The Federal Response to Hurricane Katrina: Lessons Learned.[95]
- Develop a robust corrective action process to ensure adoption of lessons identified during a review.
- Ensure scenarios involving public health threats are included in the NEP.
- Encourage greater participation in the NEP. By engaging federal, state, and local leaders, these officials will better understand their prescribed roles and the utility of their plans.
Editors
James Jay Carafano, PhD, is Vice President for the Kathryn and Shelby Cullom Davis Institute for National Security and Foreign Policy and E. W. Richardson Fellow at The Heritage Foundation. Charlotte Florance is a Policy Analyst for Africa and the Middle East in the Douglas and Sarah Allison Center for Foreign and National Security Policy, of the Davis Institute, at The Heritage Foundation. Daniel Kaniewski, PhD, is Senior Fellow in the Center for Cyber and Homeland Security at The George Washington University and Adjunct Assistant Professor in the Georgetown University School of Foreign Service. The task force chairmen, steering committee members, and participants are listed at the end of the report.
Appendix
2013–2015 Ebola Fatality Rates
The fatality rate has varied between 25 percent and 90 percent during past outbreaks. The fatality rate of the current outbreak hovered around 50 percent until mid-October 2014 when it reached 70 percent.[96] It has since plateaued, although remaining high, between 53 percent and 60 percent.[97] Appendix Table 1 shows the total numbers of confirmed cases and deaths of the 2013 outbreak as of February 2015.
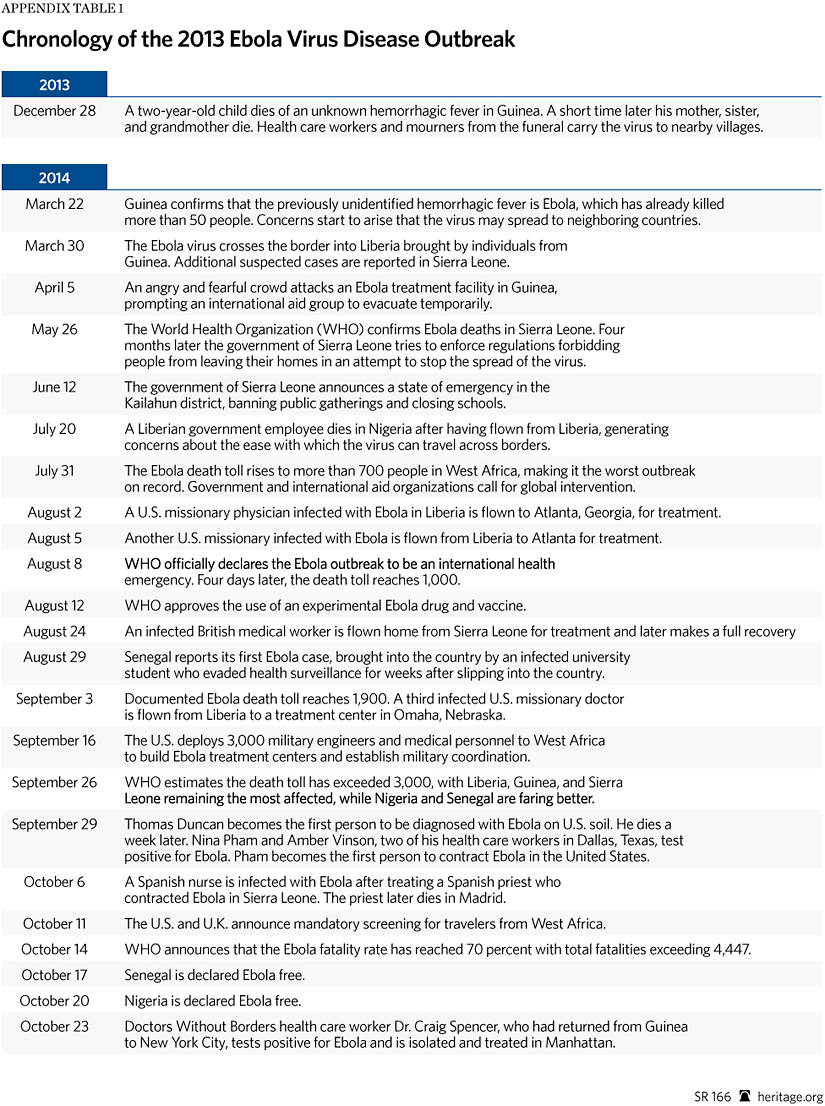
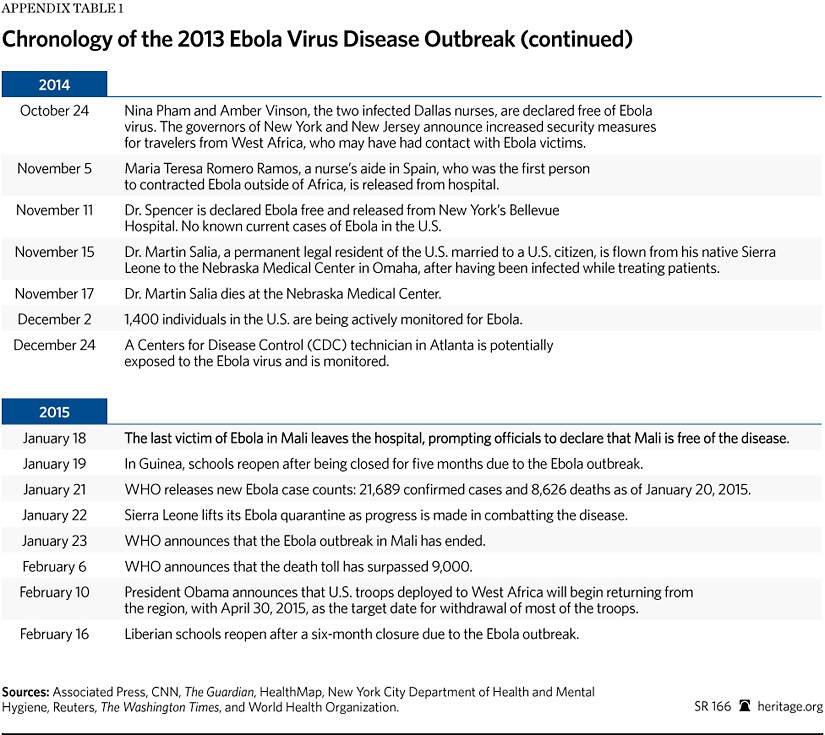
Task Force Participants
Co-Chairmen
James Jay Carafano, PhD Vice President for the Kathryn and Shelby Cullom Davis Institute for National Security and Foreign Policy, and the E. W. Richardson Fellow, The Heritage Foundation Charlotte Florance Policy Analyst for Africa and the Middle East, The Heritage Foundation Daniel Kaniewski Senior Fellow, Center for Cyber and Homeland Security, The George Washington University Adjunct Assistant Professor, Georgetown University School of Foreign ServiceSteering Committee
Paul Rosenzweig Senior Advisor, The Chertoff Group Lecturer, The George Washington University C. Stewart Verdery Jr. Founder, Monument Policy Group Senior Research Associate, Center for Strategic and International StudiesParticipants
Joshua Huminski Plans, Personnel, and Projects Coordinator, Aspen Healthcare Services Robert Kadlec Managing Director, RPK Consulting LLC Colonel Randall Larsen, USAF (Ret.) National Security Advisor, UPMC Center for Health Security Former Executive Director, Bipartisan Congressional Commission on the Prevention of Weapons of Mass Destruction Proliferation and Terrorism Matt A. Mayer Chief Operating Officer, The Liberty Foundation of America Former Senior Official, U.S. Department of Homeland Security Joshua Meservey Assistant Director, Africa Center, Atlantic Council Tibor Nagy Vice Provost for International Affairs, Texas Tech University Former U.S. Ambassador to Guinea Ha Nguyen Chief of Staff, BSA | The Software Alliance Former Advisor, U.S. Department of Homeland Security Kristjenn Nielsen President, Sunesis Consulting LLC Senior Fellow, Center for Cyber and Homeland Security, The George Washington University Chair of the World Economic Forum’s Global Council on Risk & Resilience Ryan Olson Research Associate, Center for Trade and Economics, The Heritage Foundation Elizabeth Petrun Former Associate Director, Risk Communication and Resilience Program, University of Maryland J. Peter Pham Director, Africa Center, Atlantic Council Holly Roberts Program Manager, Risk Communication and Resilience Research, University of Maryland Kristi M. Rogers Managing Director/CEO, Aspen Healthcare Services Matthew Rolfes Research Assistant, Kathryn and Shelby Cullom Davis Institute for National Security and Foreign Policy, The Heritage Foundation Tevi Troy Adjunct Fellow, Hudson InstituteSpecial Thanks
We also extend special thanks to Kirsten Bruhn, Amy Frake, Rebecca Stewart, Roman Stipić, and Jennifer Vermeulen for their research contributions.
Bibliography
Adams, Mike, “CDC Admits It Has Been Lying All Along About Ebola Transmission; ‘Indirect’ Spread Now Acknowledged,” Natural News, October 30, 2014, http://www.naturalnews.com/047457_Ebola_transmission_CDC_quackery_aerosolized_particles.html (accessed March 24, 2015).
Ahmed, Baba, “1st Ebola Case in W. African Nation of Mali,” MSN.com, October 23, 2014, http://www.msn.com/en-ca/news/other/1st-ebola-case-in-w-african-nation-of-mali/ar-BBaM3bo (accessed March 23, 2015).
Associated Press, “Ebola Death Rate Hits 70%,” New York Post, October 14, 2014, http://nypost.com/2014/10/14/ebola-death-rate-rises-above-70/ (accessed March 24, 2015).
, “Ebola Outbreak: Timeline Tracks Creeping Spread Through West Africa,” CTV News, September 16, 2014, http://www.ctvnews.ca/health/ebola-outbreak-timeline-tracks-creeping-spread-through-west-africa-1.2009572 (accessed March 24, 2015).
, “U.S. to Monitor All Travelers from 3 Nations Hit by Ebola,” The New York Times, October 22, 2014, http://www.nytimes.com/aponline/2014/10/22/us/politics/ap-us-ebola-monitoring.html (accessed March 23, 2015).
Baiz, Sylvain, et al., “Emergence of Zaire Ebola Virus Disease in Guinea,” The New England Journal of Medicine, Vol. 371, No. 15 (October 9, 2014), http://www.nejm.org/doi/full/10.1056/NEJMoa1404505 (accessed March 23, 2015).
BBC News, “Ebola Crisis: Nigeria Declared Free of Virus,” October 20, 2014, http://www.bbc.com/news/world-africa-29685127 (accessed March 23, 2015).
, “Seven Die in Monrovia Ebola Outbreak,” June 17, 2014, http://www.bbc.com/news/world-africa-27888363 (accessed March 23, 2015).
Blake, Aaron, “Americans Want Flight Restrictions from Ebola Countries. And It’s Not Close,” The Washington Post, October 14, 2014, http://www.washingtonpost.com/blogs/the-fix/wp/2014/10/14/americans-want-flight-restrictions-from-ebola-countries-and-its-not-close/ (accessed March 24, 2015).
Brown, Rob, “The Virus Detective Who Discovered Ebola in 1976,” BBC News, July 17, 2014, http://www.bbc.com/news/magazine-28262541 (accessed March 23, 2015).
Bush, George W., “Management of Domestic Incidents,” Homeland Security Presidential Directive 5, February 28, 2003, http://www.dhs.gov/publication/homeland-security-presidential-directive-5 (accessed February 18, 2015).
Centers for Disease Control and Prevention, “About Ebola Virus Disease,” http://www.cdc.gov/vhf/ebola/about.html (accessed March 23, 2015).
, “Diagnosis,” September 19, 2014, http://www.cdc.gov/vhf/ebola/diagnosis/index.html (accessed March 24, 2015).
, “Filovirus,” http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/Fact_Sheets/Filovirus_Fact_Sheet.pdf (accessed March 23, 2015).
, “Live Twitter Chat,” http://www.cdc.gov/features/twitterchat/ (accessed April 7, 2015).
, “Questions and Answers About Ebola-Reston Virus in Pigs, Philippines,” June 19, 2013, http://www.cdc.gov/ncidod/dvrd/spb/outbreaks/qaEbolaRestonPhilippines.htm (accessed April 7, 2015).
, “Signs and Symptoms,” October 18, 2014, http://www.cdc.gov/vhf/ebola/symptoms/index.html (accessed March 24, 2015).
, “What CDC Is Doing,” October 25, 2014, http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/what-cdc-is-doing.html (accessed March 25, 2015).
Chan, Margaret, “Report by the Director-General to the Special Session of the Executive Board on Ebola,” World Health Organization, January 25, 2015, http://www.who.int/dg/speeches/2015/executive-board-ebola/en/ (accessed Febch 10, 2015).
Chasmar, Jessica, “More Than 1,400 People Being Actively Monitored for Ebola in U.S.: Report,” The Washington Times, December 2, 2014, http://www.washingtontimes.com/news/2014/dec/2/more-than-1400-people-being-actively-monit/ (accessed March 24, 2015).
Cheng, Maria, “WHO Refuses to Discuss Ebola Mistakes Memo?” News.net, October 18, 2014, http://usa.news.net/article/2117403/who-refuses-to-discuss-ebola-mistakes-memo (accessed January 25, 2014).
CNN, “Ebola Fast Facts,” March 14, 2015, http://www.cnn.com/2014/04/11/health/ebola-fast-facts/ (accessed March 24, 2015).
Cooper, Colonel Thomas M., Colonel Robert C. Fulford, and Colonel Patrick T. Sullivan, “Inside the US Military’s Battle Against Ebola,” panel discussion at the Atlantic Council, Washington, DC, February 9, 2015.
Cowell, Alan, and Nick Cumming-Bruceaug, “U.N. Agency Calls Ebola Outbreak an International Heath Emergency,” The New York Times, August 8, 2014, http://www.nytimes.com/2014/08/09/world/africa/who-declares-ebola-in-west-africa-a-health-emergency.html (accessed January 25, 2014).
C-SPAN, “African Health Leadership and Ebola,” video, October 20, 2014, http://www.c-span.org/video/?322201-1/discussion-african-health-leadership-ebola&start=3324 (accessed March 24, 2015).
Davis, Rebecca, “Ebola Epidemic 2014: Timeline,” The Guardian, October 28, 2014, http://www.theguardian.com/world/2014/oct/15/ebola-epidemic-2014-timeline (accessed March 24, 2015).
De Bode, Lisa, “Ebola’s Shadow Extends to Would-Be Mecca Pilgrims,” Al Jazeera America, October 5, 2014, http://america.aljazeera.com/articles/2014/10/3/ebola-s-shadow-extendstowouldbemeccapilgrims.html (accessed March 24, 2015).
Federal Emergency Management Agency, “Emergency Support Function #8—Public Health and Medical Services Annex,” https://www.fema.gov/media-library/assets/documents/32198 (accessed February 18, 2015).
Fernandez, Manny, and Jack Healy, “With New Ebola Case Confirmed, U.S. Vows Vigilance,” The New York Times, October 15, 2014, http://www.nytimes.com/2014/10/16/us/ebola-outbreak-texas.html (accessed March 23, 2015).
Flynn, Daniel, and Stephanie Nebehay, “Aid Workers Ask Where Was WHO in Ebola Outbreak?” Reuters, October 5, 2014, http://af.reuters.com/article/topNews/idAFKCN0HU0BF20141005 (accessed January 25, 2014).
Gallagher, James, “Million Ebola Vaccine Doses for 2015, WHO Says,” BBC News, October 24, 2014, http://www.bbc.com/news/health-29756301 (accessed March 26, 2015).
Ghogomu, Mbiyimoh, “Lack of Education: The Real Reason for the Spread of Ebola,” The Higher Learning, August 17, 2014, http://thehigherlearning.com/2014/08/17/lack-of-education-the-real-reasons-ebola-is-spreading/ (accessed March 24, 2015).
Gholipour, Bahar, “American Ebola Survivors Are Likely Immune to Virus Strain Now,” Live Science, August 22, 2014, http://www.livescience.com/47511-are-ebola-survivors-immune.html (accessed March 25, 2015).
Gorman, Steve, “CDC Worker Monitored for Possible Ebola Exposure in Lab Error,” Reuters, December 25, 2014, http://www.reuters.com/article/2014/12/25/us-health-ebola-usa-idUSKBN0K21BQ20141225 (accessed March 24, 2015).
Gottlieb, Scott, and Tevi Troy, “Ebola’s Warning for an Unprepared America,” The Wall Street Journal, September 16, 2014, http://online.wsj.com/articles/scott-gottlieb-and-tevi-troy-ebolas-warning-for-an-unprepared-america-1410910044 (accessed March 24, 2015).
, “Stopping Ebola Before It Turns into a Pandemic,” The Wall Street Journal, October 3, 2014, http://online.wsj.com/articles/scott-gottlieb-and-tevi-troy-stopping-ebola-before-it-turns-into-a-pandemic-1412376544 (accessed March 24, 2015).
Grady, Denise, “Better Staffing Seen as Crucial to Ebola Treatment in Africa,” The New York Times, October 31, 2014, http://www.nytimes.com/2014/11/01/us/better-staffing-seen-as-crucial-to-ebola-treatment-in-africa.html (accessed March 25, 2015).
, “Ebola Vaccine, Ready for Test, Sat on the Shelf,” The New York Times, October 23, 2014, http://www.nytimes.com/2014/10/24/health/without-lucrative-market-potential-ebola-vaccine-was-shelved-for-years.html. (accessed October 27, 2014).
, “New Vaccines Prevent Ebola and Marburg in Monkeys,” The New York Times, June 6, 2005, http://www.nytimes.com/2005/06/06/health/06virus.html (accessed February 17, 2015).
Grady, Denise, and Sheri Fink, “Tracing Ebola’s Breakout to an African 2-Year-Old,” The New York Times, August 9, 2014, http://www.nytimes.com/2014/08/10/world/africa/tracing-ebolas-breakout-to-an-african-2-year-old.html (accessed March 23, 2015).
Gupta, Sanjay, and Danielle Dellorto, “Experimental Drug Likely Saved Ebola Patients,” CNN, August 5, 2014, http://www.cnn.com/2014/08/04/health/experimental-ebola-serum/index.html (accessed March 24, 2015).
HealthMap, “2014 Ebola Outbreaks: Timeline,” http://www.healthmap.org/ebola/#timeline (accessed February 18, 2015).
Hemingway, Mollie, “President Obama Already Has an Ebola Czar. Where Is She?” The Federalist, October 14, 2014, http://thefederalist.com/2014/10/14/president-obama-already-has-an-ebola-czar-where-is-she/ (accessed March 24, 2015).
Hinkel, Dan, Dana Ferguson, and Jon Hilkevitch, “O’Hare Among Five U.S. Airports to Beef Up Screening for Ebola,” Chicago Tribune, October 9, 2014, http://www.chicagotribune.com/news/ct-illinois-ebola-preparations-20141009-story.html (accessed March 23, 2015).
Homeland Security Council, “National Strategy for Pandemic Influenza,” November 2005, http://www.flu.gov/planning-preparedness/federal/pandemic-influenza-strategy-2005.pdf (accessed February 18, 2015).
, National Strategy for Pandemic Influenza: Implementation Plan, May 2006, http://www.flu.gov/planning-preparedness/federal/pandemic-influenza-implementation.pdf (accessed February 18, 2015).
Jones, Jeffrey M., “Americas’ Trust in Executive, Legislative Branches Down,” Gallup, September 15, 2014, http://www.gallup.com/poll/175790/americans-trust-executive-legislative-branches-down.aspx (accessed March 24, 2015).
Kanter, James, and Andrew Higgins, “Britain Pledges Millions to Fight Ebola and Chides Others to Spend More,” The New York Times, October 23, 2014, http://www.nytimes.com/2014/10/24/world/europe/britain-pledges-millions-to-fight-ebola-and-chides-others-to-spend-more.html (accessed March 24, 2015)
Keneally, Meghan, “How Ebola Emerged out of the Jungle,” ABC News, July 28, 2014, http://abcnews.go.com/Health/ebola-emerged-jungle-photos/story?id=24740453 (accessed March 24, 2015).
Lai, K. K. Rebecca, “Treating Ebola: The Hunt for a Drug,” The New York Times, October 23, 2014, http://www.nytimes.com/interactive/2014/10/23/world/africa/ebola-drugs.html (accessed October 27, 2014).
Lister, Sarah A. “Ebola: Basics About the Disease,” Congressional Research Service CRS Report, October 3, 2014, http://fas.org/sgp/crs/misc/R43750.pdf (accessed March 24, 2015).
Logistics Cluster, “Ebola Outbreak: Situation Update,” October 26, 2014, http://reliefweb.int/sites/reliefweb.int/files/resources/logistics_cluster_ebola_outbreak_situation_update_141026.pdf (accessed March 24, 2015).
Mark, Monica, “Fear and Ignorance as Ebola ‘out of Control’ in Parts of West Africa,” The Guardian, July 3, 2014, http://www.theguardian.com/world/2014/jul/02/-sp-ebola-out-of-control-west-africa (accessed March 24, 2015).
Mayo Clinic, “Ebola Virus and Marburg Virus,” August 6, 2014, http://www.mayoclinic.org/diseases-conditions/ebola-virus/basics/symptoms/con-20031241 (accessed March 24, 2015).
“Much Worse to Come,” The Economist, October 18, 2014, http://www.economist.com/news/international/21625813-ebola-epidemic-west-africa-poses-catastrophic-threat-region-and-could-yet (accessed March 24, 2015).
New York City Department of Health and Mental Hygiene, “Ebola,” October 28, 2014, http://www.nyc.gov/html/doh/html/diseases/ebola.shtml (accessed March 24, 2015).
News release, “Ebola: Most African Countries Avoid Major Economic Loss but Impact on Guinea, Liberia, Sierra Leone Remains Crippling,” The World Bank, January 20, 2015, http://www.worldbank.org/en/news/press-release/2015/01/20/ebola-most-african-countries-avoid-major-economic-loss-but-impact-on-guinea-liberia-sierra-leone-remains-crippling (accessed February 13, 2015).
News release, “More Than 16,000 Children Lost Parent or Caregivers to Ebola—Many Are Taken In by the Communities,” United Nations Children’s Fund, February 6, 2015, http://www.unicef.org/media/media_79742.html (accessed February 18, 2015).
News release, “Rep. Kelly & Sen. Rubio Introduce the Keeping Americans Safe from Ebola Act,” Office of Representative Mike Kelly (R–PA), November 20, 2014, http://kelly.house.gov/press-release/rep-kelly-sen-rubio-introduce-keeping-american-safe-ebola-act (accessed January 21, 2015).
News release, “Rubio, Colleagues Introduce Ebola Visa Ban Legislation,” Office of Senator Marco Rubio (R–FL), November 20, 2014, http://www.rubio.senate.gov/public/index.cfm/press-releases?ID=47859c11-16bc-4513-9f9c-8aa07905d694 (accessed January 21, 2015).
NPR, “Bloodmobiles to Collect Plasma from West Africa’s Ebola Survivors,” November 19, 2014, http://www.npr.org/2014/11/19/365151058/bloodmobiles-to-collect-plasma-from-west-africa-s-ebola-survivors (accessed March 25, 2015).
Obama, Barack, “Remarks by the President on Research for Potential Ebola Vaccines,” National Institutes of Health, Bethesda, Maryland, December 2, 2014, http://www.whitehouse.gov/the-press-office/2014/12/02/remarks-president-research-potential-ebola-vaccines (accessed March 24, 2015).
Park, Haeyoun, “A Cascade of Contacts from a Single Case of Ebola in Dallas,” The New York Times, October 21, 2014, http://www.nytimes.com/interactive/2014/10/20/us/cascade-of-contacts-from-ebola-case.html (accessed March 23, 2015).
PBS, “Surviving Ebola,” NOVA, October 2014, http://www.pbs.org/wgbh/nova/body/surviving-ebola.html (accessed March 23, 2015).
Rettner, Rachael, “Ebola Virus: Why Isn’t There a Cure?” TechMedia Network, June 23, 2014, http://www.livescience.com/46479-ebola-treatment-cure.html (accessed March 24, 2015).
Reuters, “Worst Ebola Outbreak on Record Tests Global Response,” October 20, 2014, http://www.reuters.com/article/2014/10/21/us-health-ebola-idUSKCN0IA00D20141021 (accessed March 24, 2015).
Robbins, Liz, Michael Barbaro, and Marc Santora, “Unapologetic, Christie Frees Nurse from Ebola Quarantine,” The New York Times, October 27, 2014, http://www.nytimes.com/2014/10/28/nyregion/nurse-in- newark-to-be-allowed-to-finish-ebola-quarantine-at-home-christie-says.html (accessed March 23, 2015).
Rodrigue, Jean-Paul, and Theo Notteboom, The Geography of Transport Systems, Hofstra University, Department of Global Studies and Geography, chap. 5, http://people.hofstra.edu/geotrans (accessed March 24, 2015).
Samb, Saliou, “Anger, Mistrust in Guinea Villages Hinders Battle to Beat Ebola,” Reuters, January 23, 2015, http://www.reuters.com/article/2015/01/23/us-health-ebola-guinea-idUSKBN0KW1ZX20150123 (accessed January 27, 2015).
Sang-Hun, Choe, “North Korea to Bar Foreign Tourists over Ebola Fears,” The New York Times, October 23, 2014, http://www.nytimes.com/2014/10/24/world/asia/north-korea-to-bar-foreign-tourists-over-ebola-fears.html (accessed March 24, 2015).
Santora, Marc, “Doctor in New York City Is Sick with Ebola,” The New York Times, October 23, 2014, http://www.nytimes.com/interactive/2014/10/23/nyregion/new-york-city-ebola-patient-timeline-map.html (accessed March 23, 2015).
Save the Children, “A Wake-Up Call: Lessons from Ebola for the World’s Health Systems,” 2015, http://www.savethechildren.org/atf/cf/%7B9def2ebe-10ae-432c-9bd0-df91d2eba74a%7D/WAKE%20UP%20CALL%20REPORT%20PDF.PDF (accessed March 10, 2015).
Schöpperle, Anna, “Analysis of Challenges of Medical Supply Chains in Sub-Saharan Africa regarding Inventory Management and Transport and Distribution,” University of Westminster, August 28, 2013, http://www.transaid.org/images/resources/Medical%20Supply%20Chain%20Challenges.Masterthesis.ASchoepperle.pdf (accessed March 24, 2015).
Sixty-Fourth World Health Assembly, “Implementation of the Internal Health Regulations (2005),” World Health Organization, May 5, 2011, http://apps.who.int/gb/ebwha/pdf_files/WHA64/A64_10-en.pdf (accessed January 25, 2014).
Sun, Lena H., et al., “Out of Control,” The Washington Post, October 4, 2014, http://www.washingtonpost.com/sf/national/2014/10/04/how-ebola-sped-out-of-control/ (accessed March 24, 2015).
U.N. Food and Agriculture Organization, “Ebola Leaves Hundreds of Thousands Facing Hunger in Three Worst-Hit Countries,” December 17, 2014, http://www.fao.org/news/story/en/item/272678/icode/ (accessed March 24, 2015).
U.N. Global Ebola Response, “Funding the Ebola Response,” http://ebolaresponse.un.org/funding-ebola-response (accessed March 13, 2015).
U.S. Department of Health and Human Services, “Office of the Assistant Secretary for Preparedness and Response (ASPR),” May 17, 2013, http://www.phe.gov/about/aspr/pages/default.aspx (accessed January 21, 2015).
U.S. Department of Homeland Security, “Enhanced Airport Entry Screening to End for Travelers from Mali to the United States,” January 5, 2015, http://www.dhs.gov/news/2015/01/05/enhanced-airport-entry-screening-end-travelers-mali-united-states (accessed January 21, 2015).
, “Enhanced Airport Security Screening to Begin for Travelers from the United States to Mali,” November 16, 2014, http://www.dhs.gov/news/2014/11/16/enhanced-airport-entry-screening-begin-travelers-united-states-mali (accessed January 21, 2015).
, “Enhanced Ebola Screening to Start at Five U.S. Airports for All People Entering U.S. from Ebola-Affected Countries,” October 8, 2014, http://www.dhs.gov/news/2014/10/08/enhanced-ebola-screening-start-five-us-airports-all-people-entering-us-ebola (accessed January 21, 2015).
United Nations Foundation, “Ebola and Public Health Impacts,” YouTube, December 2, 2014, https://www.youtube.com/watch?v=XKLi68b9UvY (accessed March 24, 2015).
“The War on Ebola,” The Economist, October 18, 2014, p. 11, http://www.economist.com/news/leaders/21625781-win-it-requires-much-larger-effort-west-africa-outside-world-has-so-far (accessed March 23, 2015).
Wasserbly, Daniel, “USMC Crisis Response Force Leader Pleased with Capability, but Warns of Limitations,” HIS Jane’s 360, February 12, 2015, http://www.janes.com/article/48954/usmc-crisis-response-force-leader-pleased-with-capability-but-warns-of-limitations (accessed February 20, 2015).
The White House, “U.S. Response to the Ebola Epidemic in West Africa,” September 16, 2014, http://www.whitehouse.gov/the-press-office/2014/09/16/fact-sheet-us-response-ebola-epidemic-west-africa (accessed March 26, 2015).
Worland, Justin, “WHO Chief Unveils Reforms After Ebola Response Criticized,” January 25, 2015, http://time.com/3681696/who-ebola-changes/ (accessed January 25, 2014).
World Bank Group, “The Economic Impact of Ebola on Sub-Saharan Africa: Updated Estimates for 2015,” January 20, 2015, http://www-wds.worldbank.org/external/default/WDSContentServer/WDSP/IB/2015/01
/19/000112742_20150119170232/Rendered/PDF/937210REVISED000Jan02002015000FINAL.pdf (accessed March 26, 2015).
, Doing Business 2015: Going Beyond Efficiency, 2014, p. 34, http://www.doingbusiness.org/~/media/GIAWB/Doing%20Business/Documents/Annual-Reports/English/DB15-Full-Report.pdf (accessed March 24, 2015).
World Health Organization, “Ebola Response Roadmap Situation Report,” December 24, 2014, http://apps.who.int/ebolaweb/sitreps/20141224/20141224.pdf (accessed March 24, 2015).
, “Ebola Response Roadmap Situation Report,” January 14, 2015, http://apps.who.int/iris/bitstream/10665/148237/2/roadmapsitrep_14Jan2015_eng.pdf (accessed March 24, 2015).
, “Ebola Situation Report,” February 11, 2015, http://apps.who.int/ebola/en/ebola-situation-report/situation-reports/ebola-situation-report-11-february-2015 (accessed March 26, 2015).
, “Ebola Virus Disease,” Fact Sheet No. 103, September 2014, http://www.who.int/mediacentre/factsheets/fs103/en/ (accessed March 23, 2015).
, “Ebola Virus Disease, West Africa (Situation as of 16 April 2014),” April 16, 2014, http://www.afro.who.int/en/clusters-a-programmes/dpc/epidemic-a-pandemic-alert-and-response/outbreak-news/4100-ebola-virus-disease-west-africa-16-april-2014.html (accessed March 23, 2015).
, “Statement on Travel and Transport in Relation to Ebola Virus Disease Outbreak,” August 18, 2014, http://www.who.int/mediacentre/news/statements/2014/ebola-travel-trasport/en/ (accessed January 21, 2015).




