High anxiety is gripping Capitol Hill. The reason: On January 1, 2014, Members of Congress and their staff will lose their current employment-based health insurance and will instead be offered coverage in the health insurance exchanges established under the new health care law.[1]
In April, Politico reported that “Congressional leaders in both parties are engaged in high-level, confidential talks about exempting lawmakers and Capitol Hill aides from the insurance exchanges they are mandated to join as part of President Barack Obama’s health care overhaul, sources in both parties said.”[2] Just hours after the Politico story broke, House Speaker John Boehner (R–OH) quickly and forcefully denied seeking an “exemption” from Obamacare, as did Senate Majority Leader Harry Reid (D–NV), while Washington Post blogger Ezra Klein rushed to explain that congressional leaders were not really seeking an “exemption” but just trying to “fix” a poorly drafted law.[3]
While Politico brought the problem out into the open, neither the original story, nor subsequent commentary from other quarters fully explained the underlying issues. Those issues include uncertainty with respect to (1) which individuals are subject to the provision; (2) when it takes effect; (3) which federal agency is responsible for administering it; and (4) how the provision will operate. Those uncertainties are mainly the result of the provision’s ambiguous wording. As Robert Pear, veteran health reporter for The New York Times, has noted, “The confusion raises the inevitable question: If they did not know exactly what they were doing to themselves, did lawmakers who wrote and passed the bill fully grasp the details of how it would influence the lives of other Americans?”[4]
Obamacare in Microcosm. Motivating any secret negotiations is a deepening concern among Members of Congress and congressional staff that they will be forced to pay more for their health care than they do today, along with the fear that the new law will impact the retention of valued employees. Those are precisely the concerns that animate millions of Americans today, especially business owners.
The uncertainty surrounding the operation and effects of a small provision in the 2010 Patient Protection and Affordable Care Act (PPACA) affecting Members of Congress heretofore attracted little attention except among a few health policy experts.[5] But that small provision provides a powerful insight into a much larger reality. Members of Congress and their staffs are facing the same problems that confront millions of employers and employees—their fellow citizens—throughout America. They will be unable to keep the health coverage they have today, and will instead be consigned to the government health exchanges, whether they like it or not. Presumably, Members and staff with other sources of coverage (such as through a spouse’s employer plan) could avoid the individual mandate penalty by enrolling in other coverage to which they have access, though they might find it less attractive than the coverage they have today. In short, Members of Congress will feel the effects of their own legislative handiwork directly.
Congressional Health Care Today
Because of the separation of powers embodied in the U.S. Constitution, the laws governing employment, pay, and benefits for employees of each of the three branches of the federal government differ somewhat and are codified in three different titles of the U.S. Code. Those applicable to officials and civilian employees of the executive branch are codified in Title 5, while those for judges and employees of the federal court system are codified in Title 28, and those for Members of Congress and legislative branch employees are codified in Title 2.
Legislative employees include not only individuals who work directly for Members of Congress, but also the staffs of congressional committees and leadership offices, and employees of the various legislative branch support offices and agencies, such as the Clerk of the House, the Secretary of the Senate, the Architect of the Capitol, the Capitol Police, the Congressional Budget Office, and the Library of Congress.
In some places, current law states that provisions applicable to the employees of one branch also apply to employees of one or both of the other two branches. That is the case with the Federal Employees Health Benefits Program (FEHBP), which is operated by the federal Office of Personnel Management (OPM) in accordance with the provisions of Title 5, Chapter 89, of the Code. While the FEHBP provides employer-sponsored health coverage principally to civilian executive branch employees, the statute defines those individuals considered federal government employees for purposes of participating in the FEHBP to include Members of Congress, federal judges, and other legislative and judicial branch employees.[6] Thus, Members of Congress and all legislative branch employees currently receive their health insurance coverage through the FEHBP.
The FEHBP operates as an employer defined-contribution plan, meaning that the employees pick the coverage they prefer from a menu of competing insurance policies and their employer (in this case the federal government) contributes an amount toward the premium. In the FEHBP, the employer contribution is set at 75 percent of the premium, up to a maximum dollar amount that is calculated and annually updated according to a formula. For 2013, the maximum FEHBP contribution amounts are $413.49 per month ($4,966.80 per year) for self-only coverage and $920.73 per month ($10,048.76 per year) for family coverage.[7]
Under the tax code, FEHBP contributions toward the cost of health care coverage are treated as tax-free income to employees—the same generous tax break enjoyed by all other Americans with employer-sponsored health insurance.
How Congress Repealed Its Own Coverage
Congress has a long and undistinguished history of exempting itself from the laws it imposes on other Americans, particularly in health care policy.[8] At the same time, various health care proposals, in and out of Congress, are sometimes framed—often erroneously—as offering the same kind of health care program that is enjoyed by Members of Congress.
In 2009, during the long and bitter congressional debate over the Obama Administration’s health care proposal, House and Senate committees addressed and disposed of numerous issues before the full Congress enacted, and the President signed into law, the mammoth Patient Protection and Affordable Care Act.
Before final enactment, the impact of the health law on Congress surfaced in the form of several key amendments. On October 28, 2009, the House Ways and Means Committee debated the House version of the legislation, which included the creation of a national “public plan” to compete against private health insurance. Representative Dean Heller (R–NV) offered an amendment that would have required Members of Congress to enroll in such a newly created “public plan” and give up their FEHBP coverage. Heller’s amendment failed, mostly along party lines, with 21 House Democrats voting “no.”[9] The House bill, however, was not the legislation ultimately signed into law. The Senate produced the version that became law.
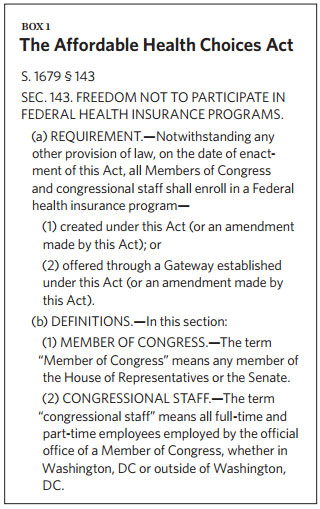
The Senate Health, Education, Labor and Pensions (HELP) Committee spent 13 days in late June and early July 2009 amending, or “marking up,” the committee’s draft health care bill. Among the hundreds of amendments offered was Amendment 226, by Senator Tom Coburn (R–OK), to require that Members of Congress and congressional staff enroll in one of the new health insurance programs created by the bill. On July 14, the committee agreed to Amendment 226 by a vote of 12 to 11. The language of that amendment appeared as Section 143 in the final bill reported by the HELP Committee to the full Senate—S. 1679, the Affordable Health Choices Act. (See Box 1.)
In late September 2009, the Senate Finance Committee marked up its own version of comprehensive health care legislation. The proposal considered by the Finance Committee did not consist of legislative text, but was a document more accurately described as a 223-page, detailed concept paper.[10] Senators on the committee filed over 550 amendments, in similar form, one of which was Amendment 328, offered by Senator Charles Grassley (R–IA), which read:
Enrollment by Members of Congress and Congressional Employees. Notwithstanding any other provision of law, beginning July 1, 2013, Members of Congress and congressional employees would be required to use their employer contribution (adjusted for age rating) to purchase coverage through a state-based exchange, rather than using the traditional Federal Employees Health Benefits Plan (FEHBP).[11]
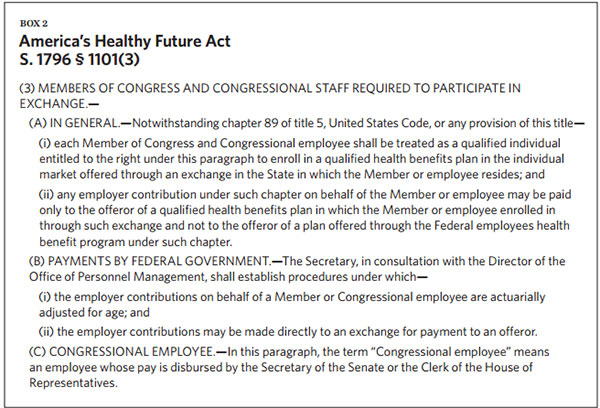
On September 29, 2009, the committee agreed to Amendment 328, “without objection.”[12] Two days later, the committee finished its mark-up and legislative drafters began turning the amended concept paper into legislative text. The final bill was reported to the full Senate as S. 1796, America’s Healthy Future Act of 2009, on October 19, 2009. Section 1101 of the act included a subsection setting forth Senator Grassley’s amendment in legislative language. (See Box 2.)
Over the next 30 days, Senate Majority Leader Harry Reid (D–NV) fashioned a new bill that was largely an amalgam of the two complex bills reported by the Finance and HELP Committees. To circumvent the constitutional requirement that all revenue-raising bills originate in the House of Representatives, Senator Reid crafted his bill as an amendment to a House-passed bill, H.R. 3590. The House bill was a measure to modify the first-time-homebuyers credit for members of the Armed Forces. Senator Reid’s amendment replaced all the original House language with the Senate health care provisions and renamed the bill the Patient Protection and Affordable Care Act.[13]
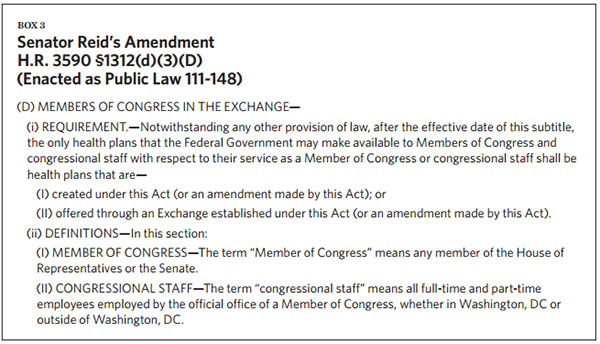
Senator Reid included language in his bill, in Section 1312(d)(3)(D), similar to that in the HELP Committee bill. (See Box 3.) The language in Section 1312 remained unchanged through the remainder of the legislative process—despite two subsequent attempts by Senator Grassley to amend it—and the provision was signed into law by President Obama on March 23, 2010, as part of the final version of H.R. 3590.
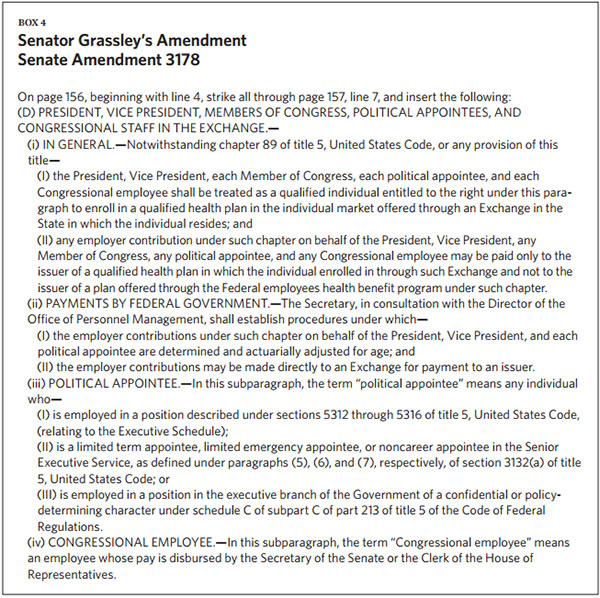
On December 11, 2009, during the Senate floor debate on Senator Reid’s version of H.R. 3590, Senator Grassley submitted Senate Amendment 3178 to replace the language in Section 1312(d)(3)(D) with the language from Section 1101(3) of S. 1796. He expanded the scope of his amendment to apply to the President, Vice President, and all executive branch political employees. (See Box 4.)[14]
The Senate debate on Majority Leader Reid’s version of the bill stretched into the Christmas season. On December 23, 2009, the Senate adopted, by a vote of 60 to 39, a cloture motion to end debate on Reid’s bill. The next day, on Christmas Eve, the Senate voted, also 60 to 39, in favor of final passage. As a result, the Senate never voted on Senator Grassley’s Amendment 3178, or on numerous other still-pending amendments.
The Senate had one more opportunity to change the language in Section 1312(d)(3)(D). On March 23, 2010, the Senate received another bill from the House, H.R. 4872, the Health Care and Education Reconciliation Act of 2010, which consisted of further amendments to the final version of H.R. 3590 that the President had just signed into law. The Senate then recommenced debate on this second installment of the health care legislation.
The next day, Senator Grassley filed Senate Amendment 3564 to H.R. 4872, containing language identical to that of his earlier Senate Amendment 3178.[15] It would have applied to the President, his cabinet, and political appointees, and would have allowed those officials, as well as Members of Congress and their staffs, to use their FEHBP employer contributions to buy coverage through an exchange. The Grassley amendment was defeated on a procedural motion by a vote of 56 to 43.[16]
Following enactment, the Office of the Law Revision Counsel codified Section 1312 into Title 42 of the U.S. Code—which deals with “The Public Health and Welfare,” and is administered by the Department of Health and Human Services (HHS).[17]
Four Key Points of Legal Ambiguity
A comparison of the provision’s final language with the alternative language of S. 1796 and Senator Grassley’s defeated floor amendments highlights four key points on which this provision of the Patient Protection and Affordable Care Act is ambiguous. Specifically:
- Applicability. While S. 1796 and the Grassley amendments applied the requirement to any employee “whose pay is disbursed by the Secretary of the Senate or the Clerk of the House of Representatives,” the enacted language applies it to congressional staff “employed by the official office of a Member of Congress.” Thus, the enacted provision could be interpreted as applying only to staff working in the personal offices of Members of Congress, in either Washington or their home state.
The imprecision of the language, say attorneys at the Congressional Research Service (CRS), raised the crucial question about whether the law would apply to staff members who work on congressional committees, or in the leadership offices, such as those of the House Speaker and Senate Majority Leader.[18] In terms of simple equity, this is a salient issue. As noted by a reporter for The Washington Post, “The vast majority of Capitol Hill staffers are assigned to personal offices, but committee and leadership staff are among the most powerful.”[19] - Enrollment in exchanges. While S. 1796 and the Grassley amendments clearly stipulated enrollment in the new exchanges by Members of Congress and congressional employees, the enacted language is vaguer, stating that “the only health plans that the Federal Government may make available to Members of Congress and congressional staff” are those offered in the exchanges.
The provision is also silent on whether the applicable exchange will be the one in Washington, D.C., or the one in a Member’s home state. The answer has both practical and political implications. If the answer is the Washington, D.C., exchange, Members would be vulnerable to public criticism that they are “out of touch” with their constituents. If the answer is the home state exchanges, Members will be covered by the different “essential benefits” packages in their respective states, further highlighting and personalizing the discriminatory effects of HHS’s essential benefits rules.[20] Yet a third option—allowing each Member to choose in which exchange to participate—could open them to the charge that they are receiving special treatment not available to their constituents. This uncertainty also affects any congressional staffers who work primarily in Washington but maintain their legal residency in their home state. - Coverage subsidy. On the crucial question of whether Members of Congress and their staff will continue to receive the employer contribution toward the cost of their coverage provided to other federal government employees, S. 1796 and the Grassley amendments are clear that they would—while the enacted language makes no such provision.
- Implementation authority. While S. 1796 and the Grassley amendments specified that HHS and OPM would coordinate the administration of the provision, the enacted language makes no such provision, and the Office of the Law Revision Counsel codified the provision into Title 42 of the U.S. Code administered by HHS. Thus, HHS is responsible for implementing the terms and conditions of congressional and staff enrollment in the exchanges and appears to also be responsible for issuing regulations defining the term “Members of Congress” and setting forth which congressional staffers are also subject to the requirement.
Yet More Ambiguity
Legislative attorneys at the Congressional Research Service analyzed those key points of ambiguity—and identified several more, all of which they detailed in an April 2, 2010, memo to Congress.[21] The additional ambiguities that the CRS identified are:
Effective Date. The CRS memo noted that “Section 1312(d)(3)(D) specifies that the section becomes effective ‘after the effective date of this subtitle,’ i.e., subtitle D of Title I of PPACA. However, given that there is no effective date applicable to the subtitle, uncertainty exists as to when § 1312(d)(3)(D) takes effect.” The CRS attorneys offered two possible interpretations; the first being that the provision took effect upon enactment, and the alternative being that the provision takes effect when the new exchanges open for enrollment. OPM subsequently adopted the second interpretation, thus permitting Members of Congress and congressional staff to continue to participate in the FEHBP through the end of the 2013 plan year.[22]
Applicability to Delegates to the House of Representatives. The CRS memo noted that the provision applies to “Members of Congress,” but does not define that term. Thus, it is unclear whether the requirement also applies to the Resident Commissioner of Puerto Rico, and the delegates from Guam, American Samoa, the U.S. Virgin Islands, the Northern Mariana Islands, and the District of Columbia. The report cites other statutes that define the terms “Members of Congress” or “Member of the House of Representatives” to explicitly include delegates and the Resident Commissioner of Puerto Rico. One such definition is in Title 5, Section 2106, which is the basis for their eligibility for coverage under FEHBP: “For the purpose of this title, ‘Member of Congress’ means the Vice President, a member of the Senate or the House of Representatives, a Delegate to the House of Representatives, and the Resident Commissioner from Puerto Rico.”[23] CRS notes that the “Supreme Court has recognized that the failure by Congress to use terms of art or specific statutory language that is normally used for certain purposes can be evidence that Congress intended a different result to apply.”
Applicability to Nontraditional Congression-al Employment Arrangements. As noted, there is considerable uncertainty with respect to which congressional employees are subject to the provision’s requirement, a point that was also addressed at length in the CRS memo. In that regard, the CRS attorneys identified further ambiguity as to the applicability of the provision to “shared staff.” A narrow interpretation could mean that a shared staffer who works for the personal offices of two Members would be treated differently than one who works for both the personal office of a Member and a committee. The CRS memo also noted similar uncertainty with respect to the provision’s application to other, nontraditional congressional employment, including contractors, consultants, congressional fellows, detailees (executive or judicial branch employees “detailed” to work for a congressional committee), and annuitants (congressional employees who previously worked for the executive or judicial branch and are entitled to FEHBP retiree coverage based on their prior service).
Conflict with “Preservation of Existing Coverage” Provision. Another issue flagged in the CRS memo is that this provision conflicts with Section 1251(a) of the PPACA, which states: “Nothing in this Act (or an amendment made by this Act) shall be construed to require that an individual terminate coverage under a group health plan or health insurance coverage in which such individual was enrolled on the date of enactment of this Act.” Yet, that provision appears to directly conflict with the requirement in Section 1312(d)(3)(D) that Members of Congress and certain congressional staff be offered only plans available in the exchanges. How the courts might rule on this conflict is highly uncertain as both of the conflicting provisions are prefaced by language asserting their primacy over other provisions. Section 1251(a) begins with the phrase “[n]othing in this Act (or an amendment made by this Act) shall be construed,” while Section 1312(d)(3)(D) begins with the phrase “[n]otwithstanding any other provision of law.”
Facing Loss of Coverage
Under the PPACA, public-sector and private-sector workers who lose their employer coverage can purchase standardized coverage in the newly created health insurance exchanges. But by losing their employer coverage, they also lose the associated—tax-free—employer subsidy for that coverage.
The effect of that shift will be mitigated somewhat for private-sector workers, whose compensation arrangements are governed by the economics of competitive labor markets. If a private employer drops coverage, he has a strong incentive to convert the funds he previously contributed to his employee health plan into higher cash wages for his workers. Otherwise, he risks losing employees to firms offering higher compensation for equivalent jobs. Labor economics holds that the conversion rate will be close to dollar for dollar. That is because what matters to the employer is the total amount of a worker’s compensation, not the relative size of the different compensation components—meaning the portion paid in cash wages versus the portions paid in the form of fringe benefits, such a health insurance or retirement plans.
However, pay and benefits of public-sector workers are set in law. Thus, for a government to “cash out” its employees’ health coverage, the applicable statute governing pay rates must be amended to permit an equivalent increase in cash wages. In the case of Members of Congress and congressional staff subject to Section 1312(d)(3)(D), unless Congress otherwise acts to increase their cash wages, their total compensation will effectively be reduced by the amount of the lost FEHBP subsidy—up to $4,966.80 per year for those with self-only coverage, or $10,048.76 per year for those with family coverage.
Thus, depending on their pay levels and current health plan choices, congressional staffers could easily face reductions in total compensation of as much as 25 percent if they lose the FEHBP subsidy without receiving equivalent wage increases. For example, in the case of a legislative aide to a House Member earning the average annual salary for that position (about $49,000) and enrolled in self-only coverage, the loss of the maximum FEHBP contribution represents a 9.2 percent reduction in total compensation. In contrast, in the case of a staff assistant earning the average annual salary for that position (about $31,000) and enrolled in family coverage, the loss of the maximum FEHBP contribution represents a 24.4 percent reduction in total compensation.
While the PPACA does provide new subsidies for coverage purchased through the exchanges, eligibility for those subsidies is restricted to set income ranges. The law provides that only individuals with household incomes between 100 percent and 400 percent of the federal poverty level qualify for federal premium subsidies in the exchanges. For 2013, the dollar amounts for those income ranges are $11,490 to $45,960 for a single individual and $23,550 to $94,200 for a family of four.
Obviously, with an annual salary of $174,000, no Member of the House or Senate will be eligible for a premium subsidy in an exchange. Most senior congressional staffers also have incomes too high to qualify for subsidies, though it is likely that many lower-paid junior staffers will be eligible for subsidies.[24] Presumably, any very low paid staff member who qualifies for Medicaid in his or her state of residence would receive Medicaid coverage instead of subsidized exchange coverage.
There is yet a further complication for many congressional staffers. Even if they meet the income test for the new exchange subsidies, their access to those subsidies depends on the outcome of two pending lawsuits. The plaintiffs in the two cases argue that the PPACA authorizes payment of the subsidies for coverage offered only in state-established exchanges—not in the “federally facilitated” exchanges set up by HHS (in states that either failed or refused to create their own exchanges).[25] Should the courts rule in favor of the plaintiffs, it would mean that the subsidies would not be available to otherwise eligible congressional staff in states with federally facilitated exchanges. Under that scenario, congressional staff residing in states with state-established exchanges (including Maryland and the District of Columbia) would receive subsidies, while those living in states with exchanges run by the federal government (including Virginia) would not.
The False Hope of an Administrative Escape
Representative Henry Waxman (D–CA), a key architect of the PPACA, says that the PPACA mandates the federal government to subsidize health plans obtained through the insurance exchanges, and that there will be no additional cost to lawmakers or their staff.[26] However, many other Members are not so confident. Senator Richard Burr (R–NC) thinks that the health law will be a “disaster” for many younger staff members, who make up about 30 percent of the Senate workforce.[27] Representative John Larson (D–CT) is hoping the problem will be resolved: “If not, I think we should begin an immediate amicus brief to say, ‘Listen, this is simply not fair to these employees.… They are federal employees.’”[28]
In short, Members and congressional staff are hoping that the Office of Personnel Management will somehow find a way to pay the FEHBP contribution to exchange plans. Once more, as reported by Politico,
[t]here have been many options for fixing the problem discussed throughout the year, including administrative fixes and legislative tweaks. One scenario seen as likely on Capitol Hill would have OPM simply decide that the government could still subsidize insurance on the exchanges. “The leadership has assured members that fixing this issue is a top priority,” said one Democratic leadership aide. “This issue must be fixed by administrative action in order that the flawed Grassley Amendment’s spirit is honored and all staff and members are treated the same.”[29]
Aside from the fact that Senator Grassley’s amendment was never enacted—and would actually have avoided the problem had it been adopted instead—congressional faith in any administrative “fix” is misplaced: There does not seem to be any way that OPM can rescue Members of Congress and their staffs.
OPM administers the FEHBP under Chapter 89 of Title 5 of the U.S. Code, and Section 8902 authorizes OPM to contract with “qualified” carriers and plan sponsors to offer health benefits plans for “uniform” (and renewable) one-year contracts. That section also confers on OPM the authority to negotiate a “detailed statement of benefits” (including definitions, limitations, and exclusions) with respect to each such contract, and sets other contracting guidelines that OPM must follow, including specifying that the rates charged be “consistent with the lowest schedule of basic rates generally charged for new group health benefit plans issued to large employers,” and that adjustment to rates at renewal be “consistent with the general practice of carriers which issue group health benefit plans to large employers.”[30]
Under 5 U.S.C. § 8906, OPM is directed to calculate the amounts of the government and employee shares of the costs of each enrollment in a health benefits plan under Chapter 89 and authorizes the employing agency to pay the government’s share per enrollment. Nowhere in Title 5 is OPM given authority to pay for an enrollment in a plan not “under this chapter” (Chapter 89)—that is, to pay the government contribution to a plan that is not one of the plans contracted for by OPM.
However, Section 1312(d)(3)(D) of the PPACA stipulates that, as of January 1, 2014, the only health insurance plans that Members of Congress and their staffs can be offered are health insurance plans “offered through an Exchange established under this Act.” Those plans are something other than OPM-negotiated plans contracted for by OPM. Furthermore, the rate and benefit requirements for exchange plans—which are individual plans, not large employer group plans—are different than those specified for FEHBP plans in 5 U.S.C. § 8902, and thus, exchange plans will not meet the standards for participating in FEHBP. Exchange plans must instead comply with the rate and benefit requirements set forth in Section 1301 of the PPACA (42 U.S.C. § 18021), which is administered by HHS.
Although OPM centrally negotiates with plan providers to participate in the FEHBP, the employer coverage contributions are actually paid on a decentralized basis by each agency from its appropriated funds. Indeed, as 5 U.S.C. § 8906(f) expressly states:
The Government contribution, and any additional payments under subsection (e)(3)(A), for health benefits for an employee shall be paid—
(1) in the case of employees generally, from the appropriation or fund which is used to pay the employee;
(2) in the case of an elected official, from an appropriation or fund available for payment of other salaries of the same office or establishment;
(3) in the case of an employee of the legislative branch who is paid by the Chief Administrative Officer of the House of Representatives, from the applicable accounts of the House of Representatives; and
(4) in the case of an employee in a leave without pay status, from the appropriation or fund which would be used to pay the employee if he were in a pay status.
The statutory framework makes it clear that the employer contributions for health benefits for Members of Congress and their staffs are to be paid from the “appropriation or fund” that is used to pay their salaries; they are not paid out of funds appropriated to OPM.
Furthermore, there is no provision in Title 41 of the U.S. Code—which codifies the statutes governing federal contracting and procurement—that supersedes the grants and limitations of OPM’s contracting authority for FEHB plans as set forth in Title 5.
Waiting for Regulations
While the lack of a statutory basis for paying the FEHBP contribution to exchange plans means that the Obama Administration cannot fix the issue of greatest concern to Congress, there are still a number of secondary issues raised by Section 1312(d)(3)(D) on which the Administration must decide, but for which it has so far not issued interpretive regulations.
OPM and Retiree Coverage. OPM retains authority to regulate matters relating to retirement benefits for retired federal workers, including Members of Congress and congressional staff. OPM might rule that congressional staffers, who based on their prior service in the executive or judicial branch qualify for FEHBP retiree coverage, would be allowed to remain in FEHBP. However, such a ruling would conflict with the “notwithstanding” clause at the beginning of Section 1312(d)(3)(D). Thus, it appears that those annuitants who are now Members or staff would not be allowed to remain in FEHBP, but might be, once they ceased to be Members or staff. The “notwithstanding” clause of Section 1312(d)(3)(D) appears on its face to strip away any entitlement that an annuitant who is now a Member or staff might have to benefits under Title 5.
HHS and Exchange Eligibility and Enroll-ment. While Members of Congress and their staffs have been looking to OPM for solutions, it is HHS that appears to be responsible for administering Section 1312, and thus resolving its other ambiguities. Specifically, regulations still need to be issued that
- Clarify in which exchanges Members of Congress are eligible to participate—those in their home state, the state in which they reside while Congress is in session (Washington, D.C., Maryland, or Virginia), or the Member’s choice;
- Determine whether non-voting delegates to the House will be treated as “Members of Congress” subject to the provision; and
- Interpret the statutory phrase “employed by the official office of a Member of Congress” to delineate which congressional staff are, and are not, subject to the provision.
Conclusion
Of course, Congress could enact legislative changes. The problem for Congress, however, is that adopting any possible legislative solution would now be viewed by many of their constituents as an act of self-dealing special treatment. Certainly, Congress has a long history of employing various legislative stratagems to “cover its tracks,” and disguise its intentions, when adopting politically unpopular laws. But, given the high degree of public attention now focused on the PPACA’s implementation, any attempt by Members of Congress to sneak a legislative fix past their constituents would be risky in the extreme.
As the legislative history shows, Congress had numerous opportunities as the PPACA made its way through the legislative process to ensure the continuation of FEHBP employer subsidies for health insurance coverage for Members and staff, and to treat committee and leadership staffs the same as Member office staffs. Yet, Congress, with support from the President, enacted a piece of legislation that rather starkly requires Members and staff to either pay for their own health insurance out of their after-tax incomes, obtain coverage under a spouse’s plan, or purchase coverage in the new exchanges (subsidized for those with family incomes that qualify). Furthermore, the provision that Congress did enact engenders more confusion than clarity with respect to both its applicability and implementation.
The fact that Members are now surprised and worried about the implications of the PPACA for themselves, and profess shock at what they enacted, leads inescapably to the question, as asked by Robert Pear of The New York Times: “If they did not know exactly what they were doing to themselves, did lawmakers who wrote and passed the bill fully grasp the details of how it would influence the lives of other Americans?”[31]
In short, Congress can keep its current health coverage by repealing Section 1312(d)(3)(D). However, the political price for doing so is that Members of Congress must repeal the rest of Obamacare as well—so that their constituents can keep their health plans, too.
—Robert E. Moffit, PhD, and Edmund F. Haislmaier are Senior Research Fellows in the Center for Health Policy Studies at The Heritage Foundation. Joseph A. Morris is an attorney in private practice and served as General Counsel of the U.S. Office of Personnel Management from 1981 to 1985.





