
Introduction
What is your doctor worth? It's simple: Payment = [{RVUws x GPCIwa} + {RVUpes x GPCIpea} + {RVUms x GPCIma}] x CF.[REF]
Unless Congress and the Administration order the government's regulatory machine to reverse gear, this baffling equation next year literally will become the basis for paying doctors in the Medicare program.
By adopting this complex system for setting physician job worth, Medicare continually will have to update arbitrary and incomprehensible "values" for thousands of different medical procedures. These, in turn, will form the basis for pricing hundreds of millions of medical services to the elderly each year. "As far as the nation's doctors are concerned," says the National Journal, "it may be the most sweeping regulatory scheme since the government imposed wage and price controls in the early 1970's."[REF]
Bureaucratic Micromanagement
As arbitrary prices continually are criticized as "unfair" by various medical specialty societies, Congress and the Administration will be pressured by physicians' groups into making innumerable "exceptions" to a mammoth set of bureaucratic rules. Thus the federal government will sink into an endless morass of bureaucratic micromanagement startlingly similar to the process of centralized economic planning now being abandoned throughout the world.
This system of price controls on physician care for the elderly will mean many doctors who feel the fees for their services are not adequate will refuse to accept Medicare patients. This will likely lead to less available care for many senior citizens. Worse, advocates of the new Medicare fee system want to impose it on the entire American health care delivery system. Just like any system of price controls, this will generate shortages in the quantity and quality of medicine for all Americans.
Incredibly, this new method of setting fees for Medicare physicians has not even been field-tested. So officials and lawmakers cannot say with any confidence what its impact will be. Nevertheless the new method of setting Medicare fees, now embodied in a 187-page Proposed Rule published in June by the Health Care Financing Administration (HCFA), the federal agency that runs the Medicare program, could revolutionize the American health care delivery system in a damaging way.
The congressionally-ordained fee schedule is called the Resource-Based Relative Value Scale (RVS), and is based on the methodology of social science rather than on market forces. Covering about 7,000 different medical procedures performed by over 500,000 physicians, the RVS system amounts to the largest single regulatory expansion in the history of the Medicare program, the huge federal health care program that services 34 million elderly citizens.
Central Planning Effort
The federal government's adoption of RVS as a mechanism to set medical prices and redistribute income among medical professionals is a remarkable historical paradox. While many nations throughout the world are rediscovering the free market and eagerly shaking off rigid and inefficient command and control economies, at the direction of Congress, the Bush Administration is preparing to impose a government-administered pricing system that will require a daunting effort of central planning on the part of the federal Health Care Financing Administration. Several lawmakers support the RVS as a model for setting fees in their proposals for national health insurance or for a mandatory employer-provided system.
Beyond its policy implications, however, more important is the likely impact of the RVS on patients. The new Medicare RVS does not even pretend to account for the "quality" or "benefit" of a medical procedure in calculating Medicare's payment to a doctor. To the contrary, the value of a medical procedure to a patient has absolutely no role whatsoever in setting the new Medicare fee. And while certain physicians will see an increase in their Medicare payments under the RVS, many others will see a sharp decrease in reimbursement for their services. Those doctors will have an incentive to make up for losses on their Medicare patients by increasing prices for their private sector patients, a process known as cost-shifting. This will further drive up already high health care costs for American businesses, employees, and their families. In fact, states William Baumol, Professor of Economics at Princeton University, "The imposition of ceilings upon the service fees charged by physicians under Medicare... would do nothing to eliminate the basic cause of rising medical care prices and would threaten to reduce the quality -- and ultimately the quantity -- of medical services available to Medicare patients."[REF]
If whole classes of physicians find their payments cut too deeply, they may be less inclined to participate in the Medicare program or take on new Medicare patients, thus undermining the availability of quality health care to the elderly, the fastest growing segment of the American population. But although policy makers know there will be an impact of this kind, they cannot make any realistic estimate of the scale or nature of the effect. The reason: In spite of the sweeping nature of this regulatory change, there have been no demonstration projects to assess the probable impact of the new Medicare fee system on doctors or patients.
Supreme Irony
By adopting the RVS, Congress and the Administration thus are trying to introduce an untested command and control approach to the problems of the American health care delivery system, rejecting market-oriented reforms. In a supreme irony therefore, the U.S. government intends in the area of health care to embrace a method of economic management that currently is being abandoned in Eastern Europe and the shattered remains of the Soviet Union. Rather than plunging further into the mire by trying to make the RVS system work, what is needed in Congress and the Administration is a fresh debate on the whole direction of health care policy. Lawmakers should seize the opportunity afforded by the discussion over the proposed RVS regulations to reopen a serious discussion of the RVS itself, including its principles, assumptions and broader implications for American health care policy. In the meantime, before ordering the federal Health Care Financing Administration to launch this unprecedented program of central planning, Congress and the Administration should pause and call a halt to the precipitous adoption of the untested Medicare Relative Value Scale. To establish some measure of predictability and cost control in Medicare physician payment, pending a full debate, federal policy makers should:
- Base future Medicare physician payment increases on the consumer price index (CPI).
- Enable patients to choose their physicians more wisely by requiring doctors to disclose all prices to patients in advance of treatment.
- Allow doctors and patients greater freedom to contract independently for Medicare services at the fees they consider appropriate.
If Congress and the Administration insist on instituting the Medicare Relative Value Scale, then at least they should follow the sound advice of Representative Michael Bilirakis, the Florida Republican, and authorize several pilot projects to field test the RVS and its impact on cost, quality, and patient access to care. A key component of such demonstration programs could be comparative analysis of the operation of the RVS system in competition with market-oriented reforms, such as a means-tested Medicare voucher program. Public policy is not an academic research project. It involves the exercise of government authority over its citizens. Before such authority is exercised, the federal government should have a much clearer idea of its implications than is the case today with the RVS.
Why RVS is an Acute Problem for Congress
The premise of the RVS is that market forces do not and cannot work in health care. The aim of the RVS system is to bring the fee structure for doctors in line with a supposedly objective standard by measuring the "value" of medical procedures. According to William Hsiao, the economist whose team at the Harvard School of Public Health developed the system, "Our relative value scale tries to mimic what the price of medical services would have been if there had been a reasonably competitive market and there had been no insurance."
For all of its vaunted scientific objectivity, however, the new payment scheme is ultimately an arbitrary system of price controls. As such, it will have the same results as any other system of price controls: distortions of demand and supply, shortages of services, cost-shifting to uncontrolled health care markets, and continuous political pressures to extend and adjust the controls. In short, the proposed RVS payments scheme will import all the problems associated with central planning. RVS advocates are not satisfied, moreover, with confining their social science experiment to the Medicare program. Many wish to see it used as the universal standard of physician payment for the entire American health care delivery system.
Doctors' Mistake
Paradoxically, lobbyists for organized medicine, led by the American Medical Association, supported congressional adoption of the new fee system two years ago. Doctors then were persuaded that the new system would mean "pay equity" within a payment system that was budget neutral, so total Medicare payments to the medical profession would be unaffected. But they have since come to recognize that they made a profound mistake.
The new medical payment rules not only are arbitrary and complex, they will mean a net loss of income for large numbers of doctors in the Medicare program. Now angry doctors are demanding that the government make changes in the regulations to restore the funding for physician reimbursement lost through the Health Care Financing Administration's (HCFA) proposed rule. Taxpayers may face new federal spending if Congress tries to restore the cuts.
The current political firestorm over the RVS regulations is reminiscent of the backlash against the Catastrophic Health Care Act of 1988, which was repealed following a storm of protest from the elderly, the very group of Americans the program was supposed to help. Opposition to the RVS rules today is coming from doctors who are supposed to be paid more fairly under the new fee system. Because of strict technical adjustments required for the new payment system, some doctors are getting lower than expected increases and while others face deeper than expected reductions. Because of strict federal budget requirements, downward adjustments in calculating physician payments by the Health Care Financing Administration will mean a reduction in total Medicare fees between $7 billion and $15 billion over the next five years.[REF]
Warned of Consequences
Lawmakers and doctors should not be shocked by the turn of events, since they were warned of the consequences of trying to introduce a complex system of price controls on physicians' services.[REF] They were told that RVS would fail to control costs, compound distortions in the health care market, create a "regulatory nightmare," and establish a radical system of government-administered pricing flatly at odds with a market economy.
The RVS fee schedule, moreover, is only one element of a three- part physician payment reform enacted by Congress. The two other related elements require the establishment of Medicare Volume Performance Standards and limits on the practice of "balanced billing" by doctors in the Medicare program.
The volume standards, which came into force in April 1990, require the Health Care Financing Administration to set an "appropriate" rate for the volume growth of Medicare's physician services. Future increases of Medicare fees then are to be based on the volume standard. In any given year, if total volume of medical services exceeds the standard, the total amount of Medicare's physician fees are to be reduced two years later.[REF]
"Balanced billing" refers to the practice of physicians charging extra amounts for treatment beyond the charge which Medicare approves. If a doctor were to charge $500 for a surgical procedure, for example, and Medicare only approves a $400 fee for that service, the doctor can collect $320 from Medicare, or 80 percent of the charge, and the patient would be responsible for the rest -- namely Medicare's 20 percent coinsurance of $80 plus the $100 billed by the doctor above the Medicare-approved fee. Under the new law, however, doctors who do not accept "assignment," that is, participate by accepting Medicare payment in full for a treatment, will not be allowed to charge more than 120 percent of the Medicare-approved charge in 1992 and no more than 115 percent in 1993. These limitations are more restrictive than previous limitations, called maximum allowable actual charges, which went into effect in 1984. By curbing balanced billing and introducing Medicare Volume Performance Standards, Congress seeks in the new law to prevent physicians from compensating for reduced Medicare fees by increasing the volume of medical services delivered to the elderly and the disabled or trying to charge fees substantially above the Medicare rates.
Mass of Data
Needless to say, trying to estimate and somehow control the total volume of Medicare services to the elderly would tax the skills of even the most sophisticated central planner. Under the 1989 statute, the Secretary of Health and Human Services, who has ultimate authority over HCFA and the new payment system, is required to collect and analyze a huge mass of data, taking into account inflation, projected increases in Medicare enrollment, the aging of the beneficiaries, the impact of technology, the availability of services to patients, and the "appropriate utilization" of Medicare.
The Health Care Financing Administration's own officials think that measuring these variables may be an almost impossible task.[REF] They believe, for instance, that volume standards are likely to be ineffective, since volume control on doctors as a whole does nothing to curtail the incentive of an individual doctor to increase his or her own volume of services.[REF] In fact, the law creates a perverse incentive for an individual doctor to increase the volume of services to prevent his or her Medicare income from declining.
Besides the enormous difficultly involved in operating the new system, its central element -- RVS -- is bad public policy because it relies on a bizarre and long-ago rejected theory of economics. Under RVS, the payment for medical services is to be based not on supply and demand but on an arbitrarily calculated value of a physician's labor, plus a calculation of the "value" of his or her practice expenses and malpractice costs weighted for geographical conditions. Relative value "units" are to be calculated for each of these factors. The value of a procedure is thus determined by a calculation of the inherent value of the variables that go into providing a medical service, but mainly the physician's labor required to provide it. The measurement of labor, in turn, includes a statistical calculation of such factors as the time and intensity of the effort required. All the variables then are to be folded into a complex formula and the procedure is given a non- monetary value relative to other procedures, which is then adjusted and is converted by a "conversion factor" to a dollar amount. Medicare fees are set accordingly. What distinguishes the RVS methodology in not the incorporation of production cost, but the attempt to set a supposedly objective non-market value on a doctor's labor.
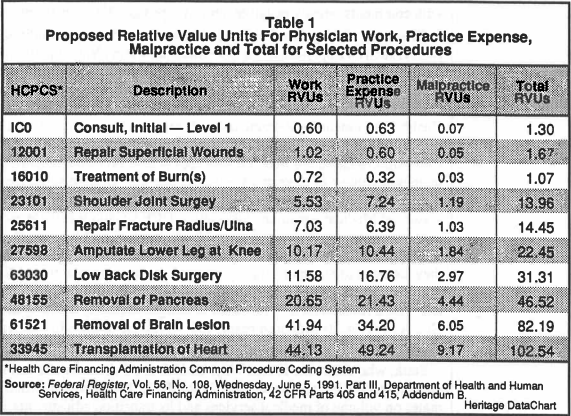
Table I provides some examples of the 4,149 different medical procedures completed thus far and how the Health Care Financing Administration ranks them according to the Relative Value Scale. A heart transplant (code 33945), for example, outranks the removal of a brain lesion (code 61521) on the relative value scale, taking into account the value calculations for work, practice expenses and malpractice costs. The law requires the Secretary of HHS to review the relative values for physicians at least every five years, but gives him flexibility to review them more frequently.
The RVS system then is not just a price control system. It is the latest version of "comparable worth," a discredited attempt to measure the value of different jobs on the basis of a social science calculation of the value of different elements of each job. Like comparable worth, it is promoted as an instrument to achieve "pay equity" in the medical profession, redistributing income from "overvalued" surgeons and diagnostic specialists, for example, to "undervalued" internists and general practitioners.
For 1992, the first year in which the RVS system will apply, Congress requires HCFA to compute the conversion factor in such a way that the aggregate Medicare payments to all doctors under the fee schedule will be the same as projected under the old system, known as "customary, prevailing and reasonable" (CPR) charges.
A storm of congressional and physician protest has greeted the Bush Administration's attempt to make the RVS work in a budget neutral fashion. Over 90,000 doctors have already flooded the Health Care Financing Administration with comments, mostly negative, on its proposed RVS regulations.
Created by Congress
Congressional leaders with responsibilities for health policy, such as Representatives Pete Stark and Henry Waxman, both California Democrats, also sharply criticize the RVS regulations, particularly HCFA's proposed 16 percent reduction in the conversion factor. This is the uniform factor in the RVS equation used to derive the final dollar amount for medical services. The Health Care Financing Administration's proposed conversion factor would reduce the amount Medicare doctors are paid over the next five years by at least $7 billion. This critical factor in computing fees is based on a bureaucratic estimate of increased volume of physicians' services resulting from lowered fees as well as certain technical adjustments necessary for the transition from the old to the new system of Medicare payment. Officials at HCFA claim that these estimates and adjustments follow a strict but reasonable interpretation of the law. In other words, if there is a problem, Congress caused it. But Administration officials also say they are open to alternative interpretations of congressional intent. Congressional critics retort that the Health Care Financing Administration's action is inconsistent with a reasonable interpretation of budget neutrality and they are pressing HCFA to revise its proposed regulations to restore billions in Medicare payments to doctors.
Stark, who chairs the House Ways and Means Subcommittee on Health, has also prepared a legislative remedy (H.R. 3070). This would override HCFA's estimates on volume of medical services and its transition adjustments, and ensure that overall payments to doctors in the Medicare program are not reduced. Under current budget law, however, Medicare spending is subject to a "pay-as-you-go" requirement. This means that any new spending must be offset by spending cuts somewhere else. But Stark's bill includes a special "declaration of emergency." This means that any new spending under his bill would be exempt from federal budget rules. Stark argues that his "emergency" legislation may be needed to save the physician "payment reform movement" and keep faith with the physician community that originally supported the Relative Value Scale.
Lost in the congressional wrangling over bureaucratic micromanagement however is the broader policy question: Why is America adopting a tool as strange as the Relative Value Scale as a central ingredient in its health care policy in the first place?
How Medicare Must Calculate the Value of Doctors' Work
According to the regulations for RVS proposed by the Health Care Financing Administration, "The relative value of each service must be the sum of the relative value units (RVU's) representing physician's work, practice expenses net of malpractice expenses, and the cost of professional liability insurance (malpractice insurance)."[REF] The regulations then require "nationally uniform" relative values for each procedure which must be adjusted by the Secretary of HHS for each locality by a "Geographical Adjustment Factor," a weighted average of geographical cost indices for the components of work, practice, and malpractice expenses.
All of these calculations are made on non-monetary values. They are changed into dollar payment amounts by the dollar conversion factor ($26.87 for fiscal 1992) for the next year. This factor is set by the Health Care Financing Administration so that the total payments for all physicians in the Medicare system will be equal to the amount already budgeted by the federal government for physician payments. Critical to keeping the fees within the federal budget is HCFA's projections of the extent to which doctors will increase their volume to offset any expected lower fees. The increasing volume and intensity of medical services has been a major force driving up Medicare costs.
Calling in Harvard
As a policy matter, budgetary adjustments are of secondary importance. The revolutionary aspect of the RVS is the attempt to discern and rank the "true" and "objective" value of physicians' services. Congress instructed the U.S. Department of Health and Human Services to hire a team of Harvard social scientists to devise such a valuation.[REF] With Congress implicitly rejecting the idea of a market-based valuation of services which determines value in the rest of the economy, the Harvard team used survey research and the statistical methods of social psychology. The objective: a scientific methodology to deduce the "true price" or a "fair and rational" price for each medical service.[REF]
The Harvard researchers quantified the various elements that go into specific medical services, ranking them according to the time and intensity, physical effort and skill, mental effort and stress expended by the doctor.[REF]
The basis for this analysis is the description of each medical procedure found in the Current Procedural Terminology (4th Edition), a compendium of medical procedures compiled by the American Medical Association. Each procedure is identified by a numerical code. Using 200 codes, a "vignette" or description of a medical service was presented to a sample of physicians, who then ranked the procedures in accordance with the "work" variables, including time and intensity, mental and physical effort, stress and skill.[REF] Using this survey analysis, relative value units (RVU's) for work were assigned for each procedure. Though the analysis ranked fewer than 400 medical procedures, the Harvard team "by extrapolation... developed physician work RVU's for about 1400 services." Thus far, the Health Care Financing Administration, in cooperation with Harvard University, has developed a total of 5,757 relative value units for medical procedures. These account for approximately 85 percent of total Medicare charges. A final part of the RVS study, due to be completed this December, will assign relative value units for remaining medical procedures and specialties.
The Harvard research team also used panels of physicians to "test whether a panel of physicians could replicate values that were generated from the national survey."[REF] The researchers claim success in these experiments, using panels of 11 to 14 physicians in each specialty. This means that setting relative values, and hence physicians fees, could become the job of small and select panels of doctors. According to the Health Care Financing Administration, this process will be used to "refine, validate, or generate" relative values for 5,000 coded medical procedures. If the Medicare RVS should be expanded to private insurance firms, either voluntarily or through national insurance, these physicians' panels would become vested with enormous political and economic power to determine the relative incomes of their fellow doctors.
Mounting Problems with the Details
Historians of economic thought will have a strong sense of dej vu as they watch the current debate on the Medicare RVS. Well over a century ago, the labor theory of value, the key component of early socialist political economy, came under relentless intellectual attack from political theorists and professional economists. As a component of socialist dogma, the labor theory of value holds that the value of a commodity or service is equal to the "socially necessary" labor time required to produce it.[REF]
Under this doctrine, the value of an item has nothing to do with the subjective value placed on it by the individual buyer, but depends solely on the effort put into producing it and some vague notion of how important the item is to society. This simple idea soon ran into serious difficulty. For one thing, "labor time" could not account for differences in skill among individual workers or classes of workers. Thus in estimating wages and prices, the practical application of the theory could not escape bitter disputes and absurd results. The Medicare RVS faces the same basic problem. As Frank Sloan, Professor of Economics at Vanderbilt University observes, " One would like to pay the talented hand surgeon a high price and the blundering hand surgeon a pittance. As a practical matter, a relative value scale cannot make this type of distinction."[REF]
Another problem was that the value of a commodity or service could not simply be determined by the average time required to produce it. Other features of work would have to be incorporated to make a wage or fee system at least superficially more rational. But the statistical ranking of occupations outside of the market cannot be a scientific process; it is essentially an arbitrary enterprise. Nevertheless, under the Harvard team, the federal government next year will attempt to operate Medicare's $44 billion Supplemental Medical Insurance program on nothing less than a reincarnation of the long-ago rejected labor theory of value.
Doctors as Lobbyists
There can be little doubt what the result will be. Each medical specialty will wrestle with every other in a never-ending struggle for taxpayers' dollars, using the rallying cries of "fairness" and "equity." Doctors will become lobbyists for their respective specialties, engaged in bitter and demeaning annual fights at the budgetary trough.
The general problems of the labor theory, detailed by economists last century, once again are emerging clearly as the Health Care Financing Administration wrestles with the details of the RVS. Like the old labor value theory, the RVS does not at all account for consumer demand or the value of a service as seen by a patient. While such variables as the physician's mental and physical effort, as well as the time of a physician's work, are factored into the equation, it has so far been impossible for architects of the system to account for either the "quality" of a medical service or the "benefit" a patient derives from it in calculating the appropriate reimbursement for a physician.
Quality and benefit, of course, are central to the issue of value, and in a market system are determined by the consumer's subjective impressions. Indeed, they cannot be determined objectively by social scientists or even a doctor. Still, RVS advocates hope that at some future date they will be able to refine their methodological techniques and develop a quality index.[REF] Meanwhile, no such indices exist, and it remains unclear how the Health Care Financing Administration is to account for them in updating regulations for RVS.
When these basic features of economic satisfaction are ignored, as they are in comparable worth systems like the RVS, the results can be strange. When the State of Washington undertook a comparable worth study of government jobs in 1974, for instance, telephone clerks outranked truck drivers, office secretaries were "valued" more than electricians, and clerical supervisors were assigned the same points as chemists.[REF]Similar oddities are now emerging in the RVS rankings of medical procedures that are reminiscent of some of the strange job comparisons that surfaced in Washington state's comparable worth tables.
Example: The use of "average time," to measure work across medical specialties results in "fifty minutes of psychotherapy" being equal to a physician "draining a finger abscess."[REF]
Example: The amount of time, effort and skill required by a doctor to treat a relatively young and healthy person normally is far less than that required to treat a frail and elderly person. But the proposed RVS regulations do not make these critical, real-life distinctions for several different kinds of surgery. Notes Edward Seljeskog, M.D., of the American College of Surgeons: "To the extent that the process for setting relative values does not reflect fully the resource inputs that are associated with the care of Medicare patients, the premise upon which the entire (RVS) system is theoretically based is violated."[REF]
Example: Patient "evaluation and management services" constitute 35 percent of "physician expenditures" in the Medicare program. The most common form of these services is a visit to the doctor's office. Office visits vary, of course. But a doctor normally spends longer time with a new patient, whose personal and medical history is unknown, than with a regular patient. The RVS formula makes no such distinction.
The Physician Payment Review Commission, the independent government commission that advises Congress on physician payments, blames such troubling examples of the RVS system on the use of "vignettes" by Harvard and the Health Care Financing Administration. The Commission criticizes these clinical scenarios used for weighing and measuring work variables as too often unrepresentative of typical situations. For example, explains the Commision, "The vignette
that was used in the Harvard project to collect resource input data for CPI [Current Procedural Terminology] code 32020 was 'Chest tube insertion for spontaneous pneumothorax in 20 year old.' Clearly, there are very few Medicare patients who fit this description. In spite of this fact, the relative value for all of the services reported under this code are based on this vignette."[REF]
Inaccurate Scenarios
Aside from inaccurate clinical scenarios describing their work, Physicians are also discovering that too many of their fellow physicians surveyed to weigh and rank the elements of medical work "rarely, if ever" performed the services to which they are assigning relative values.[REF] According to Joel Ira Franck M.D., chief of Neurosurgery at St. Mary's Hospital in Lewiston, Maine, "... one half of the chest surgeons surveyed admitted that they never perform any open-heart surgery and yet were asked to rate these services.[REF]
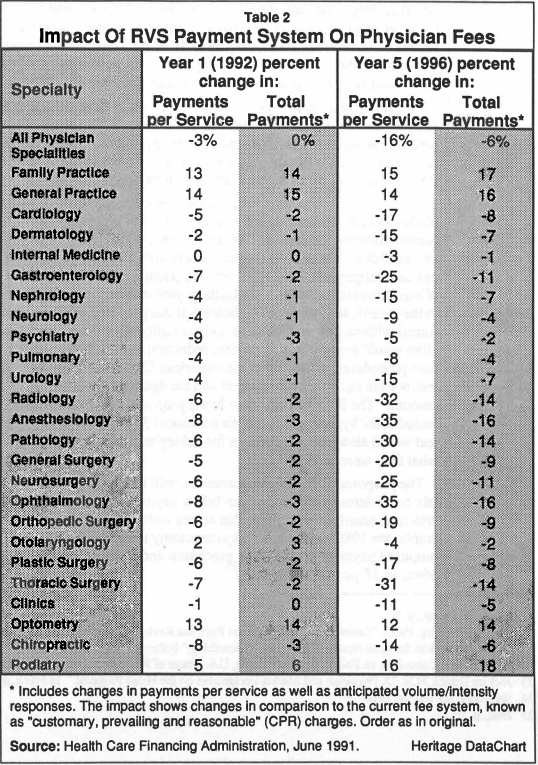
As Table II shows, the RVS system will result in some dramatic differences in doctors' fees between the old system and the new RVS system. Payment cuts are greatest for such specialties as ophthalmology, anesthesiology, radiology, and thoracic surgery. Only family practice and general practice show increases relative to the older system, by 14 percent and 15 percent, respectively.
For the past three years, Congress has been trying to control overall Medicare physician costs by combatting what it has called "overpriced procedures." But a central planning mechanism like RVS cannot adjust to constantly changing market conditions. For several medical procedures, including anesthesiology, radiology and surgery, the deep RVS cuts are coming on the heels of two straight years of significant reductions in Medicare payments enacted by Congress. According to the American College of Radiology, if the proposed RVS regulations are enforced without any modification, cuts in radiology services from 1988 through 1996 would amount to a 50 percent reduction in fees. Likewise, for coronary bypass procedures, according to the American College of Surgeons, Medicare payments were cut 9 percent last year and cut again this year by "an equal dollar amount." The RVS formula now being proposed cuts "thoracic surgery," which includes the bypass procedure, an additional 31 percent between 1992 and 1996, and would also reduce payments for kidney transplants about 50 percent below what they were in 1989.[REF]
The proposed RVS scheme moreover, will reduce payments to doctors for certain procedures in Medicare even below payments to doctors in Medicaid, the federal-state health care program that serves welfare recipients. In California, for example, the 1989 payment for a hysterectomy under Medicaid was be $810 while proposed payment for the same procedure under the new Medicare rules would be $668, an 18 percent difference.[REF]
Despite leveling such criticisms, the Physician Payment Review Commission and Washington representatives of organized medicine seem oblivious to the conceptual problems of the RVS. Instead they complain about the Bush Administration's management of physician payment reform. Thus instead of replacing the RVS with a system that would move closer to market pricing in the Medicare program, the Commission recommends another layer of bureaucratic tinkering.[REF]
An Overdose of Bureaucracy
If Congress and the Administration try to fix a system that is conceptually unsound, they will sink deeper into a mire of intricate price controls and burgeoning bureaucracy. Arbitrary and incomprehensible determinations of "values" for medical procedures will beget arbitrary and incomprehensible Medicare fees. As these are criticized by, among others, those specialty associations that can make a plausible case of "inequity" in Medicare fees, "appropriate" exceptions then will be made to the RVS system. The quest for "pay equity" will be never ending. Rules will multiply: bureaucratic micromanagement will expand relentlessly.
With its demand that the Health Care Financing Administration must find a way to make the RVS work, Congress is presenting the agency with the most daunting task of central planning its history. Not only must HCFA develop new fees, it must also monitor the volume and intensity of medical services, physician billings, and the processing of hundreds of millions of claims. It also must assure quality treatment and assure that all of this is done within the federal budget. Explains HCFA Administrator Gail Wilensky: "Whereas Medicare conducts business with 7,000 hospitals, the [RVS] program deals with almost 500,000 physicians. Rather than 11 million hospital claims to process annually, Medicare handles more than 450 million physician bills. Instead of categorizing cases into one of 475 hospital diagnostic-related groups, Medicare must contend with 7,000 codes for physician procedures."[REF]
Further Complication
Turning the RVS from theory into practice, moreover, is further complicated by Congress's specific requirement that it must be budget neutral in 1992. This is Washington jargon that means that outlays for Medicare physician payments under the new RVS system must not exceed the outlays that would have obtained under the old system of "customary, prevailing and reasonable" charges.[REF]
Under the RVS law, the computation of the conversion factor to achieve the budget target requires the Health Care Financing Administration to make predictions about how physicians will alter the volume of their services to the elderly. Difficult though this task alone would be, HCFA faces additional problems because in the transition to RVS, only about one third of the Medicare fees will be determined on the basis of the new system in 1992; the remaining payments will be made on the basis of the old payment schedule.
Therefore, two quite different payment systems will be operating in parallel. The Health Care Financing Administration thus will have to attempt to achieve budget neutrality by adjusting the RVS conversion factor in a way that tries not to only account for the volume of medical services, but also for two sets of cost increases resulting from the transition between the old and the new systems. To offset the higher than expected costs of this transition effect, HCFA intends to reduce the conversion factor by 6 percent.
Incentive to Increase Volume
Accounting for volume changes under the RVS likewise is no easy bureaucratic task. Because the new system will make lower payments to certain classes of physicians, particularly surgeons and specialists, these doctors will have an incentive to increase the volume of their services to compensate for reduced fees. According to the Congressional Budget Office, similar increases in volume entirely offset the freeze in Medicare fees in 1984-86.[REF]
Under the proposed regulations, HCFA estimates that expected physician's increase in volume of medical services would require a slightly more than a 3 percent reduction in fees to achieve budget neutrality. Again, because only about one-third of Medicare fees are under the new RVS system, the total reduction required through the conversion factor to account for these changes in volume would amount to an estimated 10 percent. With a 6 percent reduction to account for the effects of the transition to a new system and a 10 percent reduction to account for estimated increases in volume, HCFA now proposes reducing the RVS conversion factor by a total of 16 percent.
The RVS is not even in place yet, and the mounting problems of its administration are staggering. The Health Care Financing Administration is faced with all the daunting problems of instituting central planning backed by complex price controls. The agency in the future will have to keep tinkering with the RVS conversion factor or redefining the values for medical services in arbitrary ways as it attempts to get the federal budget numbers to turn out right. Miscalculations could cost taxpayers billions of dollars. In the meantime, the alleged scientific objectivity of the RVS will become nothing more than an intellectual cover for sweeping and bureaucratic price controls.
How the RVS Will Affect Patients
Controversy surrounding the proposed RVS fee schedule centers at the moment on its impact on doctors. Lost in the debate seems to be a more important consideration: its impact on the 34 million elderly Americans served by Medicare.
While access to health care is affected by many factors, such as availability of physicians in an area, a crucial factor is the willingness of doctors to treat patients. Even more important is the willingness of doctors in Medicare's parlance, to accept "assignment." Assignment is a technical term meaning a doctor's acceptance of the Medicare fee as payment in full for a medical treatment. Physicians who are designated "participating physicians" are those who accept assignment.
Since the middle of the 1980s, the number of participating physicians has climbed steadily, jumping from 28 percent of all American doctors in 1985 to 48 percent this year. Thus from the point of view of Medicare patients' access to treatment, the current system is doing very well.
"Adverse Impact"
This may change. With the new payment system, particularly the limitations on volume and "balanced billing" as well as the increasingly cumbersome and time consuming Medicare paperwork requirements, it is likely that the number of doctors willing to serve new Medicare patients will decline. While the HCFA now says it foresees no problem developing regarding access of patients to doctors willing to accept Medicare payments, in 1989 the Health Care Financing Administration told Congress that an "adverse impact on access" could be strong where fees are cut most deeply. The Health Care Financing Administration warned that "... because the changes in payment that would result under the new [RVS] fee schedule are far more extensive than previous changes, there is simply no reliable basis for predicting the response of physicians either in terms of willingness to treat Medicare patients or willingness to accept assignment."[REF]
Unlike the 1983 Prospective Payment System for hospitals, which fixed Medicare reimbursements for hospital services, the RVS payment system has not been field tested. Congress simply enacted a major change in the Medicare program without the benefit of either a pilot project or a demonstration program to test its impact.
Because of the growing dependence of physicians on Medicare for a significant portion of their practice, it is unlikely that they would simply drop large numbers of Medicare patients. More likely they will refuse to accept new patients. With the rapid growth of the aged population, this could seriously compromise patient access to care. According to the American Medical Association, the number of doctors declining to take on new Medicare patients already is on the increase, rising from 2.8 percent in 1989 to 5 percent in 1990. The largest increase has been among family practitioners.[REF]
The quantity of medical services available to the elderly is only part of the potential problem for patients. Equally important is the quality of care, something ignored by the RVS regulations. Physicians in specialties facing deep cuts in Medicare reimbursement will have less incentive to invest in innovative and cost-saving technologies or life-saving methods of treatment.
The impact of RVS on patients is also bound to go beyond the Medicare population. If the federal government sets artificially low Medicare fees for a whole class of medical specialties, doctors will have an incentive to shift costs to the non-Medicare population, meaning they will charge these patients higher prices in order to offset losses from Medicare. Such cost-shifting has occurred before when HCFA cut Medicare fees. This, of course, would aggravate the heavy inflationary pressures that already plague America's private health care delivery system.
The Lost Goal of Cost Control
The architects of the RVS, chiefly William C. Hsiao, Professor of Economics and Health Policy at Harvard University, have identified the cost of doctors services as a major cause of the high costs of American health care. The doctor is the "key decision-maker" in the health care delivery system, according to Professor Hsiao, and approximately 80 percent of all health care expenditures relating to the diagnosis, prescription, and treatment of disease are tied to decisions made by the doctor. Market forces have not been permitted to identify the price of doctors' services or to control these costs through patient decisions, so the job of the policy maker in Medicare is to find the "true price" of medical services through some arbitrary measurement of the resource costs of providing them.
Yet micromanaging doctor fees never has been able to control total costs. The reason: In Medicare it is the volume and intensity of medical services, not physicians' fees, that is the main factor driving up costs, according to officials of the Health Care Financing Administration. Thus even with the adoption of the RVS system, payments for doctors in the Medicare program still are expected to jump 63 percent over the next five years, from $27 billion in 1991 to nearly $45 billion in 1996.[REF]
If the RVS system is not going to save taxpayers much if any money, then Americans are left with nothing more than an essentially arbitrary bureaucratic calculation that one doctor's job has more or less "value" to society than another doctor's job, regardless of the subjective views of patients as to the usefulness, quality, benefit or their demand for a particular service. Taxpayers, in short, are being asked to finance a government job evaluation scheme on a class of highly paid professionals that Congress is thus far loathe to impose on any other class of American citizens.
What to do About the RVS Mess
Strangely, the Bush Administration has accepted the bizarre labor theory of value enshrined in the RVS system. It accepts the doctrine that government can and should determine the value of a person's services on the basis of supposedly objective factors. This is, of course, completely at odds with the tenets of a market economy, in which value derives from the benefit perceived by the consumer. Ironically, in his introduction to the Fiscal Year 1991 Budget, Office of Management and Budget Director Richard Darman celebrated the collapse of "state centered, command and control systems" of economic regulation, adding that "It would be a highly unfortunate irony if -- just as the world were affirming more market oriented and investment- oriented principles -- the United States were to do anything other than strengthen its commitment to these very principles."
Yet this is precisely what Darman and his Executive Branch colleagues are allowing to happen to Medicare. The RVS program is a conceptually flawed system of central planning. The whole system of payment reform is also technically flawed, according to the very officials charged with administering it.
Clean Slate
Rather than blunder into a "reform" of Medicare that is based on a long-discredited economic theory and is already triggering a political backlash reminiscent of the 1988 Catastrophic Health Care Act debacle, Congress and the Administration should wipe the slate clean and begin a thorough debate on health care reform. Such a debate should center on ways to energize consumer choice as the tool to trim medical costs while assuring the most efficient use of medical resources.[REF] While Medicare reform must be an important feature of that discussion, including the problems of malpractice and the increasingly burdensome paperwork requirements on doctors, the debate should extend to the entire heath care system.
In the meantime, Congress and the Administration should take urgent steps to avoid the dangers implicit in the RVS regulations being proposed. Among these steps:
1) Halt the introduction of the Medicare RVS.
The very adoption of a comparable worth scheme of job evaluation undermines the Bush Administration's stated commitment to a market- oriented approach to health care reform. Even for those members of Congress who do not share the Administration's commitment to markets, the proposed RVS scheme leaves unresolved too many questions about the mechanics of the new fee system and its impact on doctors and patients. Before full scale introduction of such a complex system of price controls, even proponents of the RVS approach should demand a series of demonstration projects, as a field test to determine its impact on health care quality, access and costs. More valuable still would be comparative demonstration projects, contrasting the impact of Harvard University's Physician Payment Reform plan with genuine market-oriented approaches to Medicare reform, such as Medicare vouchers.
2) Base future physician payment increases on the Consumer Price Index (CPI), with inter-specialty adjustment made by the Physician Payment Review Commission.
Physicians and patients should have some clear and understandable benchmark for Medicare payment. While the CPI is far from perfect, it is more predictable than the current convoluted payment reform system. Physician payment would be raised in line with the CPI. Within this framework, the Physician Payment Review Commission, the federal body that monitors physician reimbursement, could determine if any particular specialty is "underpaid" or "overpaid," according to whether there is an underabundance or overabundance of specialty physicians willing to take Medicare assignment. The Commission can then make specific recommendations to Congress for increases or decreases accordingly. This would be at least a rough approximation of a market system. It would also be much more flexible and far less costly than the gigantic bureaucratic effort required under the RVS system to devise update and adjust payments for 7,000 different procedures provided by 500,000 doctors.
3) Require physicians to disclose the prices of their services to Medicare patients.
Patients should be clearly informed in advance whether or not a doctor accepts assignment. If doctors will not accept assignment, or the HCFA-determined reimbursement for a specific service, then the elderly patient should be informed in writing what the service will cost before he or she is treated. The Medicare law already requires such doctors to give patients an itemized breakdown of out-of-pocket cost for elective surgery costing $500 or more. The disclosure requirement should be universal. Such a reform gives patients the opportunity to compare costs among doctors, and introduces an element of consumer-driven cost control now virtually absent from the Medicare system.
4) Coupled with mandatory price disclosure, permit balanced billing.
The new Medicare rules will prohibit a doctor should from charging a price above the amount Medicare will pay for a service. But this should be permitted, subject to the patient being informed of this in advance. An exception could be retained for Medicare Patients whose incomes fall below the poverty line. Balanced billing along with mandatory price disclosure can introduce a measure of market pressure, rewarding doctors who perform higher-quality medical services for patients who want them. According to Professors of Economics David Dranove of the University of Chicago and Mark Satterthwaite of Northwestern University, balanced billing can operate as a "safety valve that essentially guarantees access to care for most Medicare patients even if serious errors are made in the setting of Medicare fees."[REF] For market forces to operate to some degree as a constraint on prices and as a device to reward quality, consumers and providers should have greater freedom to contract with one another for services. In this connection, doctors also should be able to give patients rebates for charges below the amount Medicare sets for a service when competition would encourage it.[REF]
Conclusion
By plunging into the largest regulatory expansion in the history of the Medicare program, the Bush Administration and Congress jointly are laying the groundwork for a comprehensive system of price controls in medicine that will further distort the health care markets, undermine the credibility of the Medicare program among physicians, compromise the integrity and the independence of private medical practice, and create a regulatory nightmare.
For the Bush Administration, the adoption of the Relative Value Scale represents a dramatic departure from its stated policy goals of promoting market-oriented solutions to America's social and economic problems. For congressional lawmakers who support the RVS system, the troublesome gaps in the Health Care Financing Administration's ability to put the system into practice should indicate that it is necessary to pause and test the proposal more fully.
Full Explanation. Ordinary Americans, meanwhile, deserve a full explanation: Why does Congress assume that markets cannot work in health care delivery, and why should a significant segment of the U.S. economy be operated on the basis of principles being rejected around the world? Americans deserve some public explanation. A good, full floor debate could provide it.
Technical Difficulties. Even on its own terms, as recent testimony before Congress makes clear, the current plan for establishing the Relative Value Scale and its attendant physician payment reforms is fraught with innumerable technical difficulties. Aside from the multi-billion dollar budgetary problems resulting from the way in which the 1989 law was drafted, these technical deficiencies argue against its adoption for 1992. Without at the very least a series of demonstration projects, neither Congress nor the Administration can have any clear idea how the mix of controls will affect inflation in the medical sector or access to health care among the elderly.
Targeting physicians for price controls will not effectively solve the problem of rapidly-rising Medicare spending. Like any price control mechanism, it simply will make the situation worse. Individual physicians will have an incentive to increase the volume of their own services, regardless of a government ceiling set to reduce the aggregate amount available in the future for all doctors. Moreover, bureaucratically-imposed lower fees in Medicare will be an incentive for doctors to shift costs to the private sector, adding to the heath care costs faced by businesses and individual American paying for their own care. In all probability this will lead to pressure for extending controls to the private sector. The end result of such a policy is explicit rationing.
Soaring Medicare costs, which originally gave rise to the Medicare Relative Value Scale, are reflective of the broader problems which affect America's health care system. Dominated by third party payers, operating within a tax structure that artificially encourages employer-based insurance, the American health care system is bereft of a healthy tension between the forces of supply and demand that hold down costs elsewhere in the economy.
Market-Oriented Reforms. Genuine reform of America's health care system must begin with reform of the private sector, not Medicare. Once the system serving most Americans is put on an even keel, by strengthening consumer choice, the problems of Medicare will be much easier to solve. That does not mean that interim, short-term adjustments cannot or should not be made in the huge federal Medicare program. The most urgent of these must be to pull the plug on the Medicare Relative Value Scale. Rather than trying to set prices for hundreds of millions of Medicare transactions in an abortive attempt to outguess the market, Congress and the Administration should take the first steps toward genuine market-oriented reforms that will control health care costs and assure quality care for America's senior citizens.
Robert E. Moffit, Ph.D., Deputy Director of Domestic Policy Studies at The Heritage Foundation
© 1995 Persimmon IT, Inc.


