Early this year, Congress will work to renew welfare reform by reauthorizing the Temporary Assistance for Needy Families (TANF) program. As part of this process, Congress will also seek to reauthorize the Title V abstinence education program that was created, along with TANF, in the original 1996 welfare reform act, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA). It is expected that advocates of "safe sex" programs will use the welfare reform debate as an opportunity to push for additional federal funding for comprehensive sex education and contraception promotion programs in the name of reducing the occurrence of teen pregnancy and out-of-wedlock childbearing.
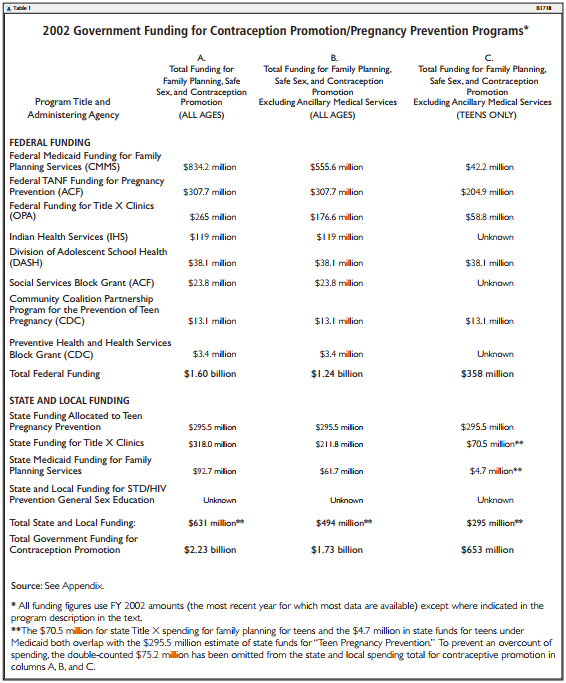
In fact, programs promoting contraceptive use already receive very large amounts of government funding. In 2002, the federal and state governments spent an estimated $1.73 billion on a wide variety of contraception promotion and pregnancy prevention programs.1 More than a third of that money ($653 million) was spent specifically to fund contraceptive programs for teens.2
By contrast, programs teaching teens to abstain from sexual activity received only an estimated $144.1 million in the same year. Overall, government spent $12 to promote contraception for every dollar spent to encourage abstinence. In addition, most contraceptive promotion or comprehensive sex-ed curricula contain material that is alarming and offensive to most parents.
This funding asymmetry seems out of line with general social priorities. Early sexual activity has harmful effects on the health, psychological well-being, and long-term life prospects of teens, and these harmful effects will be reduced only slightly by contraceptive use.
Regrettably, relatively few teens receive a clear message about the harmful effects of early sexual activity; few are taught that society expects teens to delay sexual activity. Instead, most safe sex/comprehensive sex-ed programs send the clear, if implicit, message that society expects and condones teen sexual activity. The main message is that it's okay for teens to have sex as long as they use condoms.
Any new monies devoted to preventing pregnancy should be directed not to amply funded contraception programs, but to abstinence education programs that teach teens to delay sexual activity, reveal the harm caused by casual sex with multiple partners, and help young people to prepare for fidelity, intimacy, and healthy marriage.
Government Funding for Contraceptive
Promotion and Services
Government-funded contraceptive programs promote the use of contraception for two purposes: to prevent unwanted pregnancy and to reduce the risk of infection by sexually transmitted diseases (STDs). To meet these goals, government contraceptive programs may provide contraceptive services, promote and encourage contraceptive use, or both.
A substantial amount of government funding is devoted to encouraging and facilitating contraceptive use among teens. Programs pursuing this goal are often called safe sex programs, comprehensive sex-ed programs, or STD prevention programs. These programs are also misleadingly characterized as "abstinence plus" or "abstinence first" programs although, in fact, they contain little or no abstinence content.3
Federal Funding
The federal government currently supports contraceptive programs to prevent pregnancy and STDs through eight separate funding streams. These include Medicaid; Temporary Assistance for Needy Families (TANF); Title X Family Planning; Indian Health Service funding; the Division of Adolescent School Health (DASH) of the Centers for Disease Control and Prevention (CDC); the Social Services Block Grant (SSBG); the Community Coalition Partnership Program for the Prevention of Teen Pregnancy; and the Preventive Health and Health Services Block Grant.
Medicaid Family Planning Funding
The Medicaid program is administered through the Center for Medicaid Services (CMS) in the Department of Health and Human Services (HHS). Established through the Social Security Amendments of 1965, Medicaid is the third largest source of health insurance in the United States and the largest source of funding for health-related services for America's poorest families. It is a joint federal and state program, with eligibility standards, benefits packages, payment rates, and administration established by each individual state under the same broad federal guidelines. Because it is a means-tested program, eligibility for Medicaid is based on a combination of income and resource standards.
According to federal law, the provision of family planning services and supplies is a mandatory component of the Medicaid program; such services must be provided by all states. The federal government reimburses Medicaid family planning services at a 90 percent matching rate--a rate far higher than that for most medical services. (The 90 percent matching rate means that the federal government pays for 90 percent of the costs of family planning services provided by the states through Medicaid.)
The government defines Medicaid family planning services as follows:
Family planning services are those provided to prevent or delay pregnancy or to otherwise control family size. Counseling services, laboratory tests, medical procedures, and pharmaceutical supplies and devices are covered if they are provided for family planning purposes.... Only items and pro-cedures clearly provided or performed for family planning purposes may be matched at the 90 percent rate. The 90 percent matching rate is not available for procedures that are performed for medical reasons.4
The types of contraceptive services offered through Medicaid are determined by the individual states. Currently, most state Medicaid programs offer a wide variety of contraceptive services, including oral contraceptives, condoms, diaphragms, spermicides, natural family planning, sponges, cervical cap, vaginal film, and sterilization through vasectomy or tubal ligation. In many states, Medicaid family planning funds are also used to support school-based clinics.
Medicaid is the largest source of publicly funded family planning services in the United States.5 Due to federal waivers, Medicaid funds available for family planning have increased very rapidly in the past several years, reaching $926.9 million in fiscal year (FY) 2001.6 Of this amount, 90 percent ($834 million) was federal.7 An estimated $63 million in federal funds went to pregnancy prevention and contraception services among teens.8
Calculating the cost of contraceptive services funded through Medicaid is complicated by the fact that Medicaid "family planning" charges often include such ancillary medical services as gynecological exams, pap smears, STD tests, and pregnancy tests. Medicaid rules are clear that these services are not fundable as family planning if they are provided independently or for purposes other than pregnancy prevention.
However, if these services are routinely integrated as part of the contraceptive service provided to individuals, they could be counted as family planning expenses. For example, if a clinic performs gynecological exams and pap smears as a routine procedure when providing contraceptives to individuals, these services could be included as part of overall family planning costs.
The share of overall Medicaid family planning expenditures resulting from these ancillary medical services is unknown. For purposes of this paper, we have estimated that two-thirds of Medicaid family planning costs covers contraceptives per se, while one-third covers ancillary medical services.9 Thus, excluding expenditures for ancillary services, we estimate that federal Medicaid expenditures for contraceptive services were $555 million in 2002 (two-thirds of $834 million). Expenditures for teens were $42 million. These reduced figures, excluding ancillary medical costs, are included in columns B and C of Table 1.
Temporary Assistance for Needy Families
The Temporary Assistance for Needy Families program was created as part of the 1996 Personal Responsibility and Work Opportunity Reconciliation Act. TANF is operated by the Administration for Children and Families (ACF) within the Office of Family Assistance in the Department of Health and Human Services.
One of the major goals of the TANF program is to reduce out-of-wedlock childbearing; therefore, states are free to use federal TANF funds for pregnancy prevention. According to TANF financial data, 37 states spent federal TANF funds on pregnancy prevention in FY 2002. Overall, some 2 percent of federal TANF expenditures ($323.9 million) was spent on pregnancy prevention programs in that year.10 State approaches to preventing teen pregnancy can be divided into several categories, including sex education curricula, reproductive health services, youth development programs, media campaigns, efforts to prevent repeat teen births, and multiple component interventions.
A small amount of TANF pregnancy prevention funds was spent on abstinence education. Eight states--Florida, Illinois, Kentucky, Louisiana, New Mexico, Pennsylvania, South Carolina, and Virginia--clearly describe funding of abstinence education as part of their formal TANF state plan. However, contacts with abstinence educators at the state level suggest that relatively little TANF funding is actually going to abstinence.
Based on a survey of state TANF plans and contacts with abstinence educators, we estimate that, overall, no more than 5 percent of TANF pregnancy prevention funds was channeled into abstinence education.11 On the basis of that estimate, 95 percent of federal TANF pregnancy prevention funds ($307.7 million) would have been spent on contraceptive-based pregnancy prevention, and 5 percent ($16.2 million) would have been spent on abstinence, in 2002. These figures appear in column A of Table 1.
According to the TANF Fifth Annual Report to Congress, "Most pregnancy prevention programs have focused on teenagers."12 Our analysis assumes, therefore, that two-thirds of federal TANF spending on contraceptive-based pregnancy prevention was directed to teen programs and services. This would mean that $204.9 million was spent on contraception promotion for teens through the TANF program in 2002.13 This figure appears in column C of Table 1.
Title X Family Planning
The Title X program is operated by the Office of Population Affairs (OPA) within the Office of Public Health and Science in the Department of Health and Human Services. It is the only federal program exclusively focused on the provision of family planning services on a nationwide basis. Grants are provided for voluntary family planning services through the family planning program, established by the Public Health Service Act of 1970.
Title X funds are allocated among 10 regional offices, which then award grants and monitor services among a national network of community-based clinics, state and local health departments, hospitals, university health centers, Planned Parenthood affiliates, independent clinics, and public and nonprofit agencies. The program supports a nationwide network of more than 4,600 clinics that provide reproductive health services to approximately 4.4 million people each year. In nearly 75 percent of counties in the United States, at least one provider of contraceptive services is funded by the Title X family planning program.
The program is designed to provide access to a broad range of family planning methods and services. It provides Food and Drug Administration-approved methods of contraception, contraceptive supplies, and information to all who want or need them, with priority given to low-income persons aged 15 to 44. In addition to contraceptive services and related counseling, Title X-supported clinics also provide preventive health services, including breast and pelvic examinations; cervical cancer, STD, and HIV screenings; and pregnancy testing and counseling.
Despite the fact that legal authorization for the program expired in 1985, Congress continues to appropriate money for Title X. Federal appropriations for this program for 2002 totaled $265 million.14 This figure appears in column A of Table 1. As in the case of the Medicaid program, our analysis assumes that one-third of Title X funding goes for ancillary medical services such as gynecological exams and pap smears; this would leave $177 million of federal Title X funding to promote contraception services.15 According to the U.S. General Accounting Office, roughly one-third of the program's clients are teens. Therefore, in 2002, roughly $59 million was spent on teen pregnancy prevention and contraception.16 These figures appear in columns B and C of Table 1.
Direct Health Care Services for American Indians and Alaskan Natives
Health care services for American Indians and Alaskan Natives are administered by Indian Health Services (IHS) within the Department of Health and Human Services. The IHS is responsible for providing health services to members of federally recognized tribes as part of the special government-to-government relationship between the federal government and Indian tribes. As the principal federal health care provider and health advocate for Indian people, it currently provides health services to approximately 1.5 million American Indians and Alaska Natives who belong to more than 557 federally recognized tribes in 35 states.
The IHS provides teenage pregnancy programs through a wide array of community-based services and programs. Teen pregnancy prevention activities are provided through the hospitals and clinics, as well as local community and school-based adolescent health care centers. Services provided for teens include pregnancy testing and counseling, family planning counseling, and contraceptive education.17
In 2002, out of $3.06 billion that was available for direct health care services for American Indians and Alaskan Natives, $119 million was spent on pregnancy prevention efforts.18 This figure appears in columns A and B of Table 1. It is unknown how much of that funding is specifically directed to teens, although, according to an HHS document, "Many IHS programs aim to improve the health of Indian children and adolescents."19
Division of Adolescent School Health
The Division of Adolescent School Health (DASH) is operated by the Centers for Disease Control and Prevention in the Department of Health and Human Services. DASH exists to support the development and implementation of health promotion policies and programs that address priority health risks among youth.
DASH provides funding and technical support for coordinated school health programs, HIV prevention, teen pregnancy prevention, and the prevention of STDs and other related diseases. It supports national, state, and local organizations, including national nongovernmental organizations that work with and target various populations; state and local education agencies; a nationwide network of training centers that help teachers in every state provide HIV education within coordinated school health programs; demonstration centers that train policymakers and program managers; and universities.
DASH expenditures for 2002 were $47.6 million, all of which went to programs for teens.20 Our analysis assumes that 80 percent of that sum ($38 million) went to support safe sex and contraceptive programs for teens. This figure appears in columns A, B, and C of Table 1.21
Social Services Block Grant
The Social Services Block Grant is operated through the Administration for Children and Families in the Department of Health and Human Services. The program exists to enable each state to furnish the social services that are best suited to the needs of its residents. General Block Grant funds may be used to provide services directed toward one of the following five goals specified by law: to prevent, reduce, or eliminate dependency; to achieve or maintain self-sufficiency; to prevent neglect, abuse, or exploitation of children and adults; to prevent or reduce inappropriate institutional care; and to secure admission or referral for institutional care when other forms of care are not appropriate.
The program was designed to consolidate federal assistance to states for social services into a single grant, increase state flexibility in using social service grants, and encourage each state to furnish services related to its five goals. States and other eligible jurisdictions determine their own social services programs and receive grant awards quarterly on a fiscal-year basis.
Family planning services are included in the program's goals and are defined as "educational, comprehensive medical or social services or activities, which enable individuals, including minors, to determine freely the number and spacing of their children and to select the means by which this may be achieved."22 Services available include contraceptive services, counseling and education, reproductive health care, and fertility services.
The Social Services Block Grant received $1.7 billion in 2002 appropriations, of which $23.8 million was used for pregnancy prevention programs.23 This figure appears in columns A and B of Table 1. While the amount specifically directed toward teen pregnancy prevention efforts is unknown, states are encouraged to use the funds received under this block grant to offer special services to at-risk youths.
Community Coalition Partnership Programs for the Prevention of Teen Pregnancy
Community Coalition Partnership Programs for the Prevention of Teen Pregnancy (CCPP) is operated from and funded by the Centers for Disease Control and Prevention in the Department of Health and Human Services. It is a consortium of several agencies whose aim is to reduce pregnancies among high-risk adolescents through outreach programs in 11 states among 13 different communities.24
Initiated in 1995, the program awards grants to communities in order to mobilize resources to support comprehensive teen pregnancy prevention programs. It also provides support for national nongovernmental education organizations to help schools implement teen pregnancy prevention programs.25 In FY 2002, $13.1 million was spent on community coalition pregnancy prevention programs, all of which focused on teenagers.26 This figure appears in columns A, B, and C of Table 1.
Preventive Health and Human Services Block Grant
The Preventive Health and Health Services (PHHS) Block Grant is administered through the Centers for Disease Control and Prevention in the Department of Health and Human Services. Grants awarded through this program provide states with funds to improve their residents' quality of life and reduce high-risk behaviors and activities. This program serves as the primary source of funding to states for health education and risk-reduction activities. The PHHS Block Grant provides states with flexibility to tailor disease prevention and health promotion programs to their health priority needs while enabling states to implement new programs and respond to unexpected emergencies.
The PHHS Block Grant is the primary source of flexible funding that gives states the latitude to fund any of 265 national health objectives identified in the nation's Healthy People 2010 health improvement plan, including family planning and pregnancy prevention services. Its funding is used to support, among other things, clinical services, preventive screening, laboratory support, public education, data surveillance, and program evaluation.
Because of the variance in the allowable uses of the funds, no two states allocate their block grant resources in the same way, and no two states provide similar amounts of funding to the same programs or activities. A strong emphasis is being placed on adolescents, communities with little or poor health care services, and disadvantaged populations. The states depend on this block grant to support public health funding where no other adequate resources are available.
In FY 2002, PHHS Block Grants totaled $134.9 million, a portion of which went toward pregnancy prevention efforts.27 In that year, states used $1.4 million to fund maternal and child health programs and family planning programs. Additionally, states used $2.03 million on sexually transmitted disease programs, emphasizing contraception. In total, the PHHS Block Grant provided at least $3.4 million to states for contraceptive and pregnancy prevention programs, many of which were likely to have been directed at teens, although the specific amount is unknown.28 This figure appears in columns A and B of Table 1.
State and Local Funding
State Funding for Programs to Prevent Teen Pregnancy
Many states have large-scale programs to reduce teen pregnancy that are funded by state revenues. Most of these programs focus on encouraging or facilitating contraceptive use among teens.
One survey published by the Urban Institute found that states spent $328.3 million of their own revenues on teen pregnancy prevention programs in 1999.29 The survey found that 44 states had specific policies to provide contraceptive services to teens; 28 states had specific pregnancy prevention programs in public schools. More recent data on state spending to prevent teen pregnancy are not available, but it seems unlikely that funding has fallen below the 1999 levels.
It is likely, however, that some state teen pregnancy prevention funds were used to support abstinence education. Our estimates assume that 10 percent of teen pregnancy funds went to abstinence programs, while 90 percent ($296 million) was used to support contraceptive-oriented programs and services. This figure appears in columns A, B, and C of Table 1.
State Funding for Title X Family
Planning Clinics
Title X clinics are supported by a variety of funding sources.30 In 1999, for every $1.00 received by clinics in direct federal Title X funds, state and local governments provided an additional $1.20.
Assuming that a similar spending ratio continued in subsequent years, we estimate that Title X clinics would have received $318 million in state and local funding in 2002. This figure appears in column A of Table 1. As in the case of federal Title X funds, we estimate that a third of this spending went to ancillary medical services; this would leave $212 million in state and local of funds for contraceptive services in Title X clinics.31 This figure appears in column B of Table 1.
As noted above, one-third of Title X spending is for teens. Roughly $71 million in state and local Title X contributions went to provide contraceptives to teens in 2002. This figure appears in column C of Table 1.
State Funding for Medicaid Family
Planning Services
Under the Medicaid program, states pay 10 percent of family planning costs. In 2002, state Medicaid spending on family planning came to $93 million. This figure appears in column A of Table 1. Assuming that one-third of this spending was for ancillary reproductive health services such as gynecological exams and pap smears, direct spending on contraceptive services would have been $62 million. This figure appears in column B of Table 1. Of that sum, approximately $5 million would have gone to contraceptives for teens.32 This figure appears in column C of Table 1.
State TANF Matching Funds for Pregnancy Prevention
States are required to contribute matching or "maintenance of effort" (MOE) funds to the Temporary Assistance for Needy Families program; these expenditures are financed by state rather than federal revenue. TANF financial reports for FY 2002 show that $293 million in state TANF Maintenance of Effort funds was allocated to pregnancy prevention.
These expenditures are likely to overlap considerably with state spending figures for Title X and for teen pregnancy prevention, described above. Because of the overlap, state TANF MOE spending on pregnancy prevention has not been included in the spending figures in Table 1.33
State and Local Funding for STD and HIV Prevention, Safe Sex, and General Sex Education
State governments also place a heavy emphasis on STD and HIV prevention among teens. In 1999, 41 states had a specific state policy requiring or encouraging HIV education in the public schools; 35 states required or encouraged STD education in the schools.34
Nearly all STD/HIV education programs place a heavy emphasis on encouraging contraceptive use and "safe sex." In addition, most public school systems use state and local funds to provide general sex education; most sexuality education has a contraceptive orientation. Figures on state and local funding for STD/HIV education and general sex education are not available, but given the widespread official policies supporting these programs, funding is likely to be substantial.
Abstinence Education Programs
Funding for abstinence education is far more limited and recent than funding for contraceptive services and promotion. There are only four federal programs that fund abstinence education.
Title V Abstinence Funding
A major source of abstinence funding is the Section 510 Abstinence Education Grant Program, found in Title V of the Social Security Act, established under the 1996 welfare reform legislation. Administered as block grants by the Health Resources and Services Administration (HRSA) of the Department of Health and Human Services, Title V funds provide abstinence education and, at the option of states, mentoring, counseling, and adult supervision to promote abstinence from sexual activity, with a focus on those groups who are most likely to bear children out of wedlock.
These programs encourage teen abstinence as preparation for healthy adult marriage. Grants are awarded to states based on the proportion of all low-income births in the entire country that occurred among their residents, and states can use these funds either to create abstinence education programs or to augment existing programs.
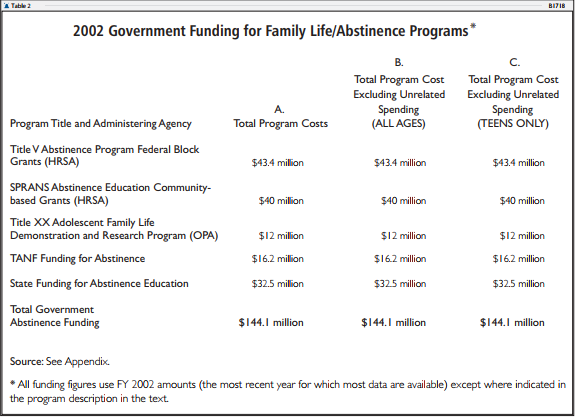
Congress authorized $50 million per year in Title V grants for FY 1998 through FY 2002.35 However, as California has consistently elected not to receive Title V funds, actual spending has been less than that amount. In 2002, the federal government spent a total of $43.4 million to fund Title V abstinence programs.36 This figure appears in columns A, B, and C of Table 2.
In 1999, states provided direct service to 1.28 million young people with Title V funds; two-thirds of these clients were age 14 or younger. The low numbers of high school students receiving abstinence education is in line with the states' apparent practice of focusing primarily on contraceptive promotion in high schools.37
SPRANS Abstinence Funding
Funding for abstinence programs is also available through the Title V Special Projects of Regional and National Significance (SPRANS) program, administered by the Health Resources and Services Administration of the Department of Health and Human Services. Included in SPRANS is the Community-based Abstinence Education Project Grant Program, which provides direct grants for public and private entities to develop and implement abstinence-only education programs for adolescents of ages 12 through 18 in communities throughout the United States.
In FY 2002, SPRANS received $40 million for the Abstinence Education Project Grant Program. This sum was increased to $55 million in FY 2003.38 This figure appears in columns A, B, and C of
Table 2.
Title XX Adolescent Family Life Demonstration and Research Program
In addition, abstinence education funding is available through the Title XX Adolescent Family Life Demonstration and Research Program in the Office of Population Affairs within the Office of Public Health and Science in the Department of Health and Human Services. Enacted in 1981 as part of the Public Health Services Act (P.L. 97-35), Title XX provides funding for a variety of adolescent health programs.
Total funding for Title XX in FY 2002 was $28.9 million. Of this amount, only an estimated $12 million was directed toward teen abstinence programs.39 This figure appears in columns A, B, and C of Table 2.
TANF Funding for Abstinence
As noted previously, states spent $323.9 million of federal TANF funds on pregnancy prevention in FY 2002. Based on a review of state TANF plans and contacts with abstinence leaders, we estimate that approximately 5 percent of that sum ($16.2 million) went to abstinence education. This figure appears in columns A, B, and C of Table 2.
State Funding for Abstinence
State governments are required to match federal funding for the Title V abstinence program at a 75 percent rate. Funding from any source--state, local, or private--can be used in the match.
Abstinence educators report that a large portion of Title V matching funds takes the form of in-kind contributions made by local abstinence organizations backed by private donations. Our analysis assumes, however, that state funding for abstinence in 2002 was roughly $32.5 million, or 75 percent of federal funding for Title V. This figure appears in columns A, B, and C of Table 2.
Overall Spending On Pregnancy Prevention, Safe Sex, and Contraception Promotion Compared to Abstinence
Overall spending totals are shown in both Tables 1 and 2. Total government spending allocated to family planning, pregnancy prevention, safe sex, and contraceptive promotion was approximately $2.23 billion in 2002.40 However, these figures are likely to be substantially below real expenditure totals, since figures on state and local spending on STD/HIV prevention and general sex education are not available. Individual program spending figures are shown in column A of Table 1.
As noted in the prior discussion, accurate spending estimates are complicated by the fact that some portion of family planning spending in the Medicaid and Title X programs goes to ancillary medical services such as gynecological exams and pap smears. We have attempted to adjust for this in column B of Table 1. In that column, federal and state spending totals for Medicaid and Title X have been reduced by one-third to exclude estimated costs of ancillary medical services. After this adjustment, total government spending on pregnancy prevention, safe sex, and contraceptive promotion is estimated to have been $1.73 billion in 2002.
Expenditures on teens, with a similar adjustment, are shown in column C of Table 1. After adjustment, total spending on teens for pregnancy prevention, safe sex, and condom promotion is estimated to have been $653 million in 2002. Summary spending figures are shown in Chart 1.
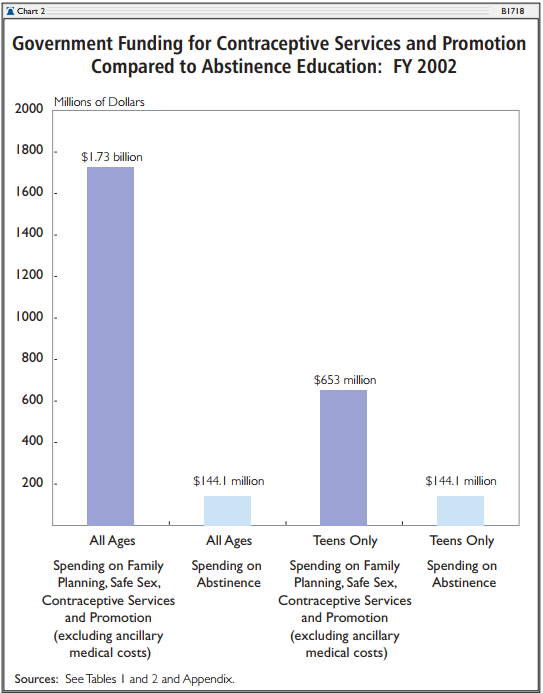
An overall comparison of spending on pregnancy prevention and safe sex compared to abstinence is shown in Chart 2. Total government spending on family planning, safe sex, and contraceptive promotion (after the exclusion of funding for ancillary medical services and non-related expenditures) was $1.73 billion for adults and teens combined. By contrast, total spending for abstinence was only $144.1 million. Thus, the government spent $12 on contraception services and promotion for each dollar spent on abstinence.
A similar disparity exists in funding for teens. Total government spending on family planning, safe sex, and contraceptive promotion for teens (after the exclusion of funding for ancillary medical services and non-related expenditures) was $653 million. By contrast, total spending for teen abstinence was only $144.1 million. Thus, the government spent nearly $4.50 on contraception services and promotion for teens for each dollar spent on abstinence.
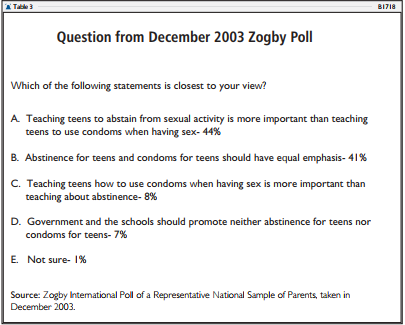
However, these spending priorities are exactly the opposite of what parents in the United States say they want taught to their teens. In a recent Zogby poll, only 8 percent of parents surveyed said they believe that teaching teens how to use a condom is more important than teaching teens to abstain from sexual activity. Instead, an overwhelming majority--85 percent--of parents said that the emphasis placed on abstinence for teens should be equal to or greater than the emphasis placed on contraception. (see Table 3).41
Uncertainties in Estimates
The figures in Table 1 involve a number of uncertainties. The largest of these is the share of Medicaid and Title X family planning funding that goes to ancillary medical services such as gynecological exams and pap smears. These procedures are often treated as essential components of the provision of contraceptives. Therefore, they could reasonably be included as a component of the overall cost of contraceptive services.
However, our analysis has assumed that ancillary medical costs represented one-third of total family planning costs in the Medicaid and Title X programs, and we excluded these ancillary medical costs from the contraceptive spending totals in columns B and C of Table 1 and from the comparisons in Chart 2. Others may estimate that the costs of these ancillary services are higher or lower than our figures.
A second major uncertainty or inaccuracy is the absence of figures for state and local spending on HIV/STD prevention and general sex education.42 This sum is likely to be considerable, but information is not available at the present time.
Other smaller uncertainties exist. The amount of TANF funding directed to abstinence education is uncertain, as is state and local funding for abstinence. However, contacts with abstinence educators suggest that the funds received from these sources are limited.
Clearly, it would be possible to produce estimates for contraceptive and abstinence spending that are somewhat higher or lower than the figures in Tables 1 and 2. However, no matter how the figures were adjusted, it would be extremely difficult to produce figures that contradicted the primary finding that government funding for contraceptive services and promotion is many times greater than funding for abstinence education.
For example, if spending on ancillary medical services were assumed to be two-thirds of family planning totals in the Medicaid and Title X programs, rather than one-third as our analysis assumes, total government spending on contraception would still remain at $1.36 billion and $603 million for teens. The overall spending figure would be still be 10 times higher than spending on abstinence, and the teen spending figure would still be four times higher.
Efforts to Expand Contraceptive Funding
Despite the large current imbalance between contraceptive funding and abstinence funding, strong efforts exist to further expand contraceptive funding and to reduce or eliminate funding for abstinence. For example, as part of the welfare reform reauthorization process, Representative Henry Waxman (D-CA) joined with many other liberals on the House Energy and Commerce Committee in an unsuccessful effort to abolish the existing Title V abstinence education program and replace it with new sex education funding that state bureaucracies could use for either safe sex or abstinence programs. Since the public health bureaucracies that would control the allocation of these funds are largely wedded to the "safe sex" approach and are hostile to abstinence education, the net effect of this legislative change, had it been enacted, would have been to eliminate a substantial portion of the abstinence education funds that are currently available.
Similarly, the Family Life Education Act (H.R. 3469), sponsored by Representative Barbara Lee (D-CA), seeks to provide $100 million per year in new funding for "comprehensive sexuality education" programs. Advocates of this type of legislation often try to solicit support by claiming that safe sex or comprehensive sex-ed programs support abstinence. They frequently mislabel these programs as "abstinence plus" or "abstinence first" curricula.
These terms, however, are very misleading; most "abstinence plus" curricula contain little or no abstinence content.43 Typically, comprehensive sex-ed curricula contain only a few token sentences on abstinence in a text devoted almost exclusively to promoting condom use. In reality, most of these curricula convey the message that society expects and condones widespread teen sexual activity; none conveys the message that society expects young people to avoid sexual activity throughout their teen years.
Another effort to expand funding for contraceptive education is the Work and Family Act,44 co-sponsored by Senators Evan Bayh (D-IN) and Tom Carper (D-DE). This bill would provide $50 million to states' contraceptive programs to prevent teen pregnancy. The bill's contraceptive programs are labeled "abstinence first." However, as noted above, safe sex curricula are habitually passed off as "abstinence" curricula because they contain a few token references to abstinence. Advocates of the Bayh-Carper legislation have been unable to explain how "abstinence first" programs would differ from existing comprehensive sex-ed/safe sex programs.
Finally, as part of his overall TANF reauthorization bill, the Work, Opportunity and Responsibility for Kids Act (WORK) Act, Senator Max Baucus (D-MT) included a new program to provide $50 million per year in funding for safe sex and contraception education. The sex education provisions of this bill closely followed those of the Bayh-Carper Work and Family Act. The Baucus WORK bill was passed by the Senate Finance Committee in the summer of 2002 but was never brought to the Senate floor.
Sex-Ed Curricula Materials Deeply Offensive to Parents
As noted above, given the popularity of abstinence education among parents, safe sex and comprehensive sex-ed programs are often misleadingly labeled "abstinence plus" or "abstinence first." Advocates of these curricula will disingenuously assert they are pro-abstinence because they contain a few perfunctory references to abstinence among materials that are overwhelmingly devoted to encouraging contraceptive use.
In addition, safe sex/comprehensive sex-ed curricula generally contain materials that are deeply offensive to most parents. Most government-funded safe sex programs contain explicit demonstrations of contraceptive use, especially condoms. Often, comprehensive sex-ed programs require middle school students to practice unrolling condoms on dildos or bananas, and they have students practice shopping for condoms.
For example, the sex education program "Focus on Kids" teaches middle school and high school students that "there are other ways to be close to a person without having sexual intercourse.... The list may include body massage, bathing together, masturbation, sensuous feeding, fanaticizing watching erotic movies, reading erotic books and magazines."45 This program is widely promoted by the Centers for Disease Control.
Another well-known "abstinence plus" sex-ed curriculum promoted at the CDC is "Be Proud! Be Responsible!" This curriculum has students engage in homosexual role-playing; it also encourages middle school and high school students to "think up a sexual fantasy using condoms" and to "use condoms as a method of foreplay." Students as young as 13 years old are taught to "act sexy/sensual when putting condoms on, hide them on your body and ask your partner to find it" and "tease each other manually while putting the condom on."46
Another aggressively promoted CDC "abstinence-plus" program, "Becoming a Responsible Teen (B.A.R.T.)," has students practice putting condoms on a plastic phallus. In addition, students receive instruction about using condom lubricants and are told to "find something around the house or at a convenience store to use as a substitute." If they "don't have a water-based lubricant handy," they are told that "grocery store lubricants...grape jelly, maple syrup, and honey" can serve as substitutes.47
Conclusion
Early sexual activity has manifold harmful effects. Teens who are sexually active are more likely to be depressed and are more likely to attempt suicide.48 Beginning sexual activity at a young age greatly increases the probability of becoming infected with sexually transmitted diseases. Girls who begin sexual activity at an earlier age are far more likely to have abortions.49
Women who begin sexual activity at an early age are far more likely to become pregnant and give birth out of wedlock and to be single mothers. Since single mothers are far more likely to be poor, early sexual activity is linked to higher levels of child and maternal poverty.50
Early sexual activity seriously undermines the ability of girls to form stable marriages as adults. When compared to women who began sexual activity in their early 20s, girls who initiated sexual activity at ages 13 or 14 were less than half as likely to be in stable marriages in their 30s. Beginning sexual activity at an older age, however, is linked to higher levels of personal happiness in adult years.51
Abstinence education programs seek to encourage a delay in sexual activity.52 Abstinence is widely popular, and many evaluations show that abstinence education programs can substantially reduce teen sexual activity. Despite this, there is currently relatively little government funding for abstinence education.
Total government spending for abstinence was only $144.1 million in FY 2002. By contrast, total government spending on family planning, safe sex, and contraceptive promotion was $1.73 billion in the same year. In other words, the government spent $12 on contraception services and promotion for each dollar spent on abstinence.
A similar disparity exists in funding for teens and youth. In FY 2002, government spending on family planning, safe sex, and contraceptive promotion for teens was $653 million. By contrast, total spending for teen abstinence was only $144.1 million. Thus, the government spent nearly $4.50 on contraception services and promotion for teens for each dollar spent on abstinence.
This term, the Senate will act to renew welfare reform by reauthorizing TANF. This legislation will also include reauthorization of the Title V abstinence program. As part of TANF reauthorization, it is likely that some in the Senate will seek to establish new funding for safe sex/contraceptive promotion programs. Given the alarming content of most comprehensive sex-ed programs, and given the current funding imbalance between contraceptive promotion and abstinence, efforts to increase contraceptive programs for teens would be dangerously counterproductive.
Melissa G. Pardue is Harry and Jeanette Weinberg Fellow in Social Welfare Policy in the Domestic Policy Studies Department, Robert E. Rector is Senior Research Fellow in Domestic Policy Studies, and Shannan Martin is Research Assistant in Welfare Policy at The Heritage Foundation.
Spending Calculations
Medicaid: Federal Family Planning Funding
Medicaid spending on family planning has expanded very rapidly in recent years due to federal waivers that have allowed states to expand the number of beneficiaries. In FY 2000, Medicaid expenditures on family planning were $577.6 million; of that total, 7.6 percent went to services for youth. See Table 7 at www.dhhs.state.sc.us/NR/rdonlyres/ea5iyls55hidbqvgvj3amti6
uqke4cbibb2nnyd3m5y5n4ic3qlxn27u4lsvcdapbmol bv6yjozpcj/208200partial.pdf. According to preliminary internal Center for Medicaid Services (CMS) documents provided by congressional staff, total Medicaid family planning expenditures rose to $926.9 million in FY 2001. (These documents are available from the authors upon request.) Of this amount, some 90 percent ($834.2 million) was federal spending; this figure appears in column A of Table 1. Our analysis assumes that one-third of Medicaid family planning spending goes to ancillary medical services, leaving two-thirds ($555.6 million) for contraceptive services in 2001. Of the total of $555.6 million, we estimate that some $42.2 million (7.6 percent) went to services to teens, based on historic spending patterns.
Federal TANF Funding for Pregnancy Prevention (ACF)
According to 2002 TANF Financial Data available at www.acf.dhhs.gov/programs/ofs/data/tableA_break_2002.html, $323.9 million (2 percent of total federal TANF expenditures) was spent on pregnancy prevention efforts. Our estimate assumes that 95 percent of this funding goes to contraceptive promotion and 5 percent to abstinence education ($307.7 million and $16.2 million, respectively). According to the TANF Fifth Annual Report to Congress, "Most pregnancy prevention efforts have focused on teenagers." The estimate of $204.9 million in funding for contraception for teens in column C of Table 1 assumes that 66.6 percent of $307.7 million in TANF contraceptive funds went to teens.
Federal Funding for Title X Clinics (OPA)
According to the Office of Family Planning in the Office of Population Affairs at the Department of Health and Human Services, federal funding for the Title X program was $265 million in FY 2002. See http://opa.osophs.dhhs.gov/titlex/ofp-funding-history.html. Our estimate assumes that one-third of Title X funding was used for ancillary medical services, leaving $176.6 million available for contraception promotion; this figure appears in column B of Table 1. Estimated funding for teens appears in column C of Table 1. According to the General Accounting Office, approximately one-third of the program's funding is for teens. See Teen Pregnancy: State and Federal Efforts to Implement Prevention Programs and Measure Their Effectiveness, GAO/HEHS-99-4, November 1998, p. 34. See also "Background on the Federal Title X Program," Republican Study Committee Policy Brief, April 2003, at www.house.gov/burton/RSC/TitleX03PB.doc. One-third of $176.6 million is $58.8 million, spent on teen pregnancy prevention. See also "Surveillance of Family Planning Services at Title X Clinics and Characteristics of Women Receiving These Services, 1991," at www.cdc.gov/epo/mmwr/preview/mmwrhtml/00053549.htm.
Division of Adolescent School Health (DASH)
Funding for the DASH program in FY 2002 was $47.6 million, all of which went to programs for teens. Our estimate assumes that 20 percent of DASH funding went to general reproductive health services, leaving $38 million available for contraception promotion programs for teens. See www.cdc.gov/nccdphp/dash/index.htm. See also Republican Study Committee, "2002 Federal Sex-Ed/Contraception vs. Abstinence Funding," September 6, 2002, at www.house.gov/burton/RSC/Abstinence4.PDF.
Social Services Block Grant (ACF)
The Social Services Block Grant received $1.7 billion in 2002 appropriations, of which $23.8 million was used for pregnancy prevention programs. While the amount specifically directed to teen pregnancy prevention efforts is unknown, states are encouraged to use this money to offer special services to at-risk youth. See "2002 Federal Sex-Ed/Contraception vs. Abstinence Funding" at www.house.gov/burton/RSC/Abstinence4.PDF.
Community Coalition Partnership Program for the Prevention of Teen Pregnancy (CDC)
According to the CDC, $13.1 million was spent on pregnancy prevention programs in 2002 under the Community Coalition Partnership program. All of this funding was directed to programs for teenagers. See www.cdc.gov/nccdphp/drh/up_adolpreg.htm.
Preventive Health and Health Services Block Grant (CDC)
According to figures available at www.cdc.gov/nccdphp/blockgrant/hp2010.htm, states spent roughly $3.4 million in Preventive Health and Health Services Block Grant funds on contraceptive services and related programs in FY 2002. This sum includes $2.03 million on programs to prevent sexually transmitted diseases (the majority of which are contraception promotion programs); $882,893 on family planning services; and $518,390 on Maternal, Infant, and Child Health programs. No data were available to determine what proportion of that funding was spent on teen contraception promotion.
State Funding Allocated to Teen Pregnancy Prevention
According to a study published by the Urban Institute, states reported spending $328.3 million of their own revenues on teen pregnancy prevention in 1999. See Richard Wertheimer, Justin Jager, and Kristin Moore, "State Policy Initiatives for Reducing Teen and Adult Nonmarital Childbearing: Family Planning to Family Caps," November 2000, at www.urban.org/UploadedPDF/anf_a43.pdf. More recent data are not available. Our estimate assumes that 10 percent of these funds may go to abstinence education, leaving $295.5 million (in column B of Table 1) for programs with a contraceptive focus.
State Funding for Title X Clinics
Title X clinics are supported by a variety of funding sources. In 1999, Title X grantees reported $737.9 million in total revenues. Of that sum, 25 percent came directly from the federal Title X program, 12 percent came from other federal sources, 14 percent came from Medicaid reimbursements, 29 percent came from state and local governments, and 20 percent came from patient fees and other sources. See "Government Performance Result Act (GPRA)" at http://opa.osophs.dhhs.gov/titlex/ofp_references.html.
In 1999, for every $1.00 received by clinics in direct federal Title X funds, state and local governments provided an additional $1.20. Our estimates assume that a similar spending ratio continued in subsequent years. This means that Title X clinics would have received $318 million in state and local funding in 2002. As in the case of federal Title X funds, we estimate that a third of this spending went to ancillary medical services. This would leave $212 million in state and local funds for contraceptive services in Title X clinics. This figure appears in column B of Table 1. As noted above, one-third of Title X spending is for teens. Roughly $71 million in state and local Title X contributions went to provide contraceptives to teens in 2002.
State Medicaid Funding for Family Planning Services
Medicaid spending on family planning has expanded very rapidly in recent years due to federal waivers that have allowed states to expand the number of beneficiaries. According to preliminary internal CMS documents provided by congressional staff, total Medicaid family planning expenditures rose to $926.9 million in FY 2001. Of this total, 10 percent ($92.7 million) was state spending; this figure appears in column A of Table 1. Our analysis assumes that one-third of Medicaid family planning spending goes to ancillary medical services, leaving two-thirds ($61.7 million) for contraceptive services in 2001. Of that $61.7 million total, we estimate that some $4.7 million (7.6 percent) went to services to teens based on historic spending patterns.
Total Spending figures for Contraception Promotion
The figures for total state spending on contraception promotion are slightly less than the sum of the individual program totals because of overlap in the funding for some individual programs. Specifically, the $70.5 million for state Title X funding for teens and the $4.7 million for state Medicaid funding for teens overlap with the $295.5 million in "State Funds Allocated to Teen Pregnancy Prevention." Consequently, the duplicated amount of $75.2 million has been subtracted from all the spending totals in columns A, B, and C of Table 1.
Title V Abstinence Program Federal Block Grants (HRSA)
See Section 510 of Title V fact sheet at ftp://ftp.hrsa.gov/mchb/abstinence/statefs.pdf.
SPRANS Abstinence Education Community-based Grants (HRSA)
See SPRANS Community-based Abstinence Education Project Grant Program fact sheet at
ftp://ftp.hrsa. gov/mchb/abstinence/cbofs.pdf.
Title XX Adolescent Family Life Demonstration and Research Program (OPA)
According to the Office of Adolescent Pregnancy Programs, total funding in FY 2002 for Title XX was $28.9 million. The estimate assumes that only $12 million of those funds was spent on abstinence programs, all of which are directed at teens. See http://opa.osophs.dhhs.gov/titlexx/oapp-funding-history.html.
According to 2002 TANF Financial Data available at www.acf.dhhs.gov/programs/ofs/data/tableA_break_ 2002.html, $323.9 million (2 percent of total federal TANF expenditures) was spent on pregnancy prevention efforts. Our estimate assumes that 5 percent of this funding ($16.2 million) went to abstinence education.
State Funding for Abstinence Education
The figure $32.55 million equals the state match in the Title V abstinence funds (75 percent of federal Title V spending). This figure is also consistent with our assumption that some 10 percent of the $328.3 million in state funds for pregnancy prevention went to abstinence. See "State Funding Allocated to Teen Pregnancy Prevention," above.
1. For a detailed description of funding sources, see Table 1 and Appendix. Unless otherwise noted, FY 2002 figures were used in all cases because they were the most accurate and comprehensive data available.
2. See Republican Study Committee, "2002 Federal Sex-Ed/Contraception vs. Abstinence Funding," September 6, 2002, at www.house.gov/burton/RSC/Abstinence4.PDF.
3. See Advocates for Youth, "The Future of Sexuality Education: Science or Politics?" Transitions, Vol. 4, No. 3 (March 2001), p. 4.
4. Chryl Andrews and Tracey Orloff, State Medicaid Coverage of Family Planning Services, National Governors' Association, December 1995, p. 2 (emphasis in original).
6. Total family planning expenditures for FY 2001 are according to preliminary internal CMS documents provided by congressional staff. Documents are available upon request from the authors. See also Medicaid information in Appendix.
7. In Table 1, the federal Medicaid expenditures for family planning ($834.2 million) and state Medicaid expenditures ($92.7 million) are presented separately.
8. Based on Medicaid's FY 2000 report, which shows that 7.6 percent of Medicaid family planning expenditures went to fund services for youth. The estimate of $63 million for teen services in 2001 assumes that the 7.6 percent share of family planning spending is relatively constant and would apply to 2001 spending as well. See Table 7, "Medicaid Expenditures--Fiscal Year 2000," at www.dhhs.state.sc.us/NR/rdonlyres/ea5iyls55hidbqvgvj3amti6uqke4cbibb
2nnyd3m5y5n4ic3qlxn27u4lsvcdapbmolbv6yjozpcj/208200partial.pdf.
9. The authors have been unable to obtain information on the share of Medicaid family planning funds allocated to ancillary medical services and would welcome further research or information on this topic to better understand the allocation of resources.
10. See U.S. Department of Health and Human Services, Administration for Children and Families, FY 2002 TANF Financial Data, at www.acf.dhhs.gov/programs/ofs/data/tableA_break_2002.html. TANF financial reports also show $293 million in pregnancy prevention spending as part of state Maintenance of Effort spending under TANF. These expenditures, financed by state rather than federal revenue, are likely to overlap with state spending figures for Title X and for teen pregnancy prevention described below. For this reason, we have excluded them in the spending figures in Table 1. See www.acf.dhhs.gov/programs/ofs/data/tableB1_2002.html.
11. The authors are engaged in an ongoing communication with abstinence leaders in order to obtain a firmer estimate of TANF funding for abstinence.
14. See Office of Family Planning, "Funding History Table, FY 1971-2002", at http://opa.osophs.dhhs.gov/,titlex/ofp-funding-history.html.
15. The authors have been unable to obtain information on the specific allocation of Title X funds and would welcome further research or information on the breakdown of Title X funds in order to better understand where the resources are being spent.
16. See U.S. General Accounting Office, Teen Pregnancy: State and Federal Efforts to Implement Prevention Programs and Measure Their Effectiveness, GAO/HEHS-99-4, November 1998, p. 34. See also "Background on the Federal Title X Program," Republican Study Committee Policy Brief, April 2003, at www.house.gov/burton/RSC/TitleX03PB.doc.
19. Federal Grants Manual for Youth Programs: A Guide to Youth Risk Behavior Prevention Funding, Vol. I, U.S. Department of Health and Human Services, 1999, p. 227.
21. See www.cdc.gov/nccdphp/dash/index.htm.
22. Federal Grants Manual for Youth Programs: A Guide to Youth Risk Behavior Prevention Funding, Vol. I, p. 114.
24. For a list of the 13 communities, see www.cdc.gov/reproductivehealth/tpartner.htm.
25. See National Campaign to Prevent Teen Pregnancy, "Breaking Ground: Lessons Learned from The Centers for Disease Control and Prevention's Community Coalition Partnership Programs for the Prevention of Teen Pregnancy," December 2003 at www.teenpregnancy.org/resources/data/pdf/BreakingGround.pdf.
26. See Advocates for Youth information on CCPP at www.advocatesforyouth.org/publications/coststudy/investments.htm. See also Republican Study Committee, "2002 Federal Sex-Ed/Contraception vs. Abstinence Funding."
27. See National Center for Chronic Disease Prevention and Health Promotion, "Preventive Health and Health Services Block Grant: PHHS Block Grant Appropriations History," at www.cdc.gov/nccdphp/blockgrant/history.htm.
28. See "Preventive Health and Health Services Block Grant: National Allocation of Funds by Healthy People, 2000/2010 Health Problem," at www.cdc.gov/nccdphp/blockgrant/hp2010.htm.
29. Richard Wertheimer, Justin Jager, and Kristin Moore, "State Policy Initiatives for Reducing Teen and Adult Nonmarital Childbearing: Family Planning to Family Caps," Urban Institute New Federalism Paper, Series A, N. A-42, November 2000, at www.urban.org/UploadedPDF/anf_a43.pdf.
30. In 1999, Title X grantees reported $737.9 million in total revenues. Of that sum, 25 percent came directly from the federal Title X program, 12 percent came from other federal sources, 14 percent from Medicaid reimbursements, 29 percent from state and local governments, and 20 percent from patient fees and other sources. See U.S. Department of Health and Human Services, Office of Population Affairs, Office of Family Planning, "OFP References: Government Performance Results Act (GPRA),"at http://opa.osophs.dhhs.gov/titlex/ofp_references.html.
31. As noted previously, the authors have been unable to obtain information on the specific allocation of Title X funds and would welcome further research or information on the breakdown of Title X funds to clarify how resources are being spent.
33. See U.S. Department of Health and Human Services, Administration for Children and Families, FY 2002 TANF Financial Data, at www.acf.dhhs.gov/programs/ofs/data/tableB1_2002.html.
35. See U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau, fact sheet, "Section 510 Abstinence Education Grant Program," April 2002, at ftp://ftp.hrsa.gov/mchb/abstinence/statefs.pdf.
37. U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau, 2000 Annual Summary for the Abstinence Education Provision of the 1996 Welfare Law P.L. 104-193, Section 510 of Title V of the Social Security Act, July 2002, at ftp://ftp.hrsa.gov/mchb/abstinence/annualrpt00.pdf.
39. See U.S. Department of Health and Human Services, Office of Population Affairs, Office of Adolescent Pregnancy Programs, "Funding History Table, FY 1982-2002," at http://opa.osophs.dhhs.gov/titlexx/oapp-funding-history.html.
40. The estimates for total spending on family planning, safe sex, and contraceptive promotion in columns A, B, and C of Table 1 are complicated by the fact that there is overlap in the spending figures for state and local programs. Specifically, both state spending on teens in the Title X program ($70.5 million) and state spending on teens in Medicaid ($4.7 million) are likely to be duplicated in the overall category of "state funds allocated to teen pregnancy prevention." To avoid duplicate counting, state spending on teens in Title X and Medicaid (a total of $75.2 million) has been subtracted from the government spending totals in columns A, B, and C of Table 1. Consequently, the total spending figures will be slightly less than the sum of the individual program totals.
41. Zogby International Poll of a representative national sample of parents, taken in December 2003.
42. Most sex education in the United States that is not explicitly abstinence education has a strong contraceptive orientation.
43. Based on a forthcoming Heritage Foundation content analysis of comprehensive sex-ed, "abstinence plus," and "abstinence first" curricula.
45. Physicians Consortium, "Sexual Messages in Government-Promoted Programs and Today's Youth Culture," April 2002.
48. Robert E. Rector, Kirk A. Johnson, Ph.D., and Lauren R. Noyes, "Sexually Active Teenagers Are More Likely to Be Depressed and to Attempt Suicide," Heritage Foundation Center for Data Analysis Report No. 03-04, June 3, 2003.




